Theodore Loftsgard APRN, ACNP, CCRN
Adam Frost RRT, CRT
Dacia Evans RN
Karen Kolbet PharmD, RPh
Division of Critical Care
Mayo Clinic
Rochester, Minnesota
History of Present Illness
A 55 year old woman was transferred to the ICU from the general medicine ward for tachycardia and acute hypoxic respiratory distress. She has multiple myeloma and had received cycle one of bortezomib, dexamethasone, thalidomide, cisplatin, doxorubicin, cyclophosphamide and etoposide (VDT-PACE) and radiotherapy to T7 for a pathologic compression. She was admitted for pain control from mucositis.
Past Medical History
In addition to the multiple myeloma she has a past medical history of asthma, ovarian cysts, diverticulitis, eczema, pneumonia, laparoscopic cholecystectomy, total abdominal hysterectomy with bilateral salpingo-oophorectomy, appendectomy, ectopic pregnancy in the past, and left Bell's palsy.
Current Medications
- Acyclovir 400 mg BID
- Albuterol 90 HFA prn
- Allopurinol 300 mg daily
- Fluconazole 200 mg BID
- Gabapentin 300 mg BID,
- Hydromorphone
- Levofloxacin 500 daily
- Morphine
- Omeprazole
- Bactrim 400-80 mg daily for PCP prophylaxis
- Thalomid 200 mg capsule daily
- Ativan 0.5 mg just prior to transfer
Physical Examination
- Vital Signs: temperature 36.4 °C, respiratory rate 24 breaths/minute, blood pressure 148/77 mm Hg, pulse 133/minute, SpO2 98% on oxygen at 4 L/min.
- General: Alert and follows commands. Slightly somnolent. In respiratory acute distress.
- Skin: Pink, warm and dry without acute rashes or lesions.
- Eyes: EOMs intact. Conjunctivae pink. Sclerae anicteric
- ENT: Neck supple. Trachea midline.
- Cardiac: S1, S2 irregular rate and rhythm without extra sounds, murmurs, rubs or gallops. Capillary refill 2 seconds.
- Lungs: Respirations with accessory muscle use, shallow. scattered crackles and equal to auscultation. Diminished bilateral bases.
- Abdomen: Soft. No abdominal tenderness. Non-distended. Bowel sounds present.
- Extremities: Peripheral pulses +2/4 throughout. 1+ peripheral edema.
- Neuro: GCS = 13, residual bell's palsy.
Pertinent Labs
- Sodium: 144 mmol/L
- Potassium: 4.2 mmol/L
- Chloride: 113 mmol/L *
- Bicarbonate,: 23 mmol/L
- Creatinine: 0.6 mg/dL
- Hematocrit: 20.5 %
- Leukocytes: 0.5 x10(9)/L
- Hemoglobin: 6.2 g/dL
- Platelet Count: 39 x10(9)/L
- Calcium, Ionized(S): 4.81 mg/dL
- pH (FOR CALCIUM, IONIZED [S]): 7.47
- INR: 1.5
- APTT(P): 29 sec
Her ECG (Figure 1) showed a tachycardia with a maximum heart rate was in the 170's.
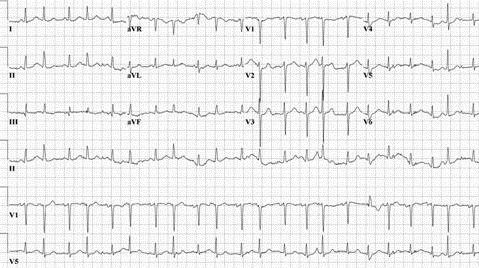
Figure 1. Admission ECG to the ICU.
Her admission chest x-ray is shown in Figure 2.
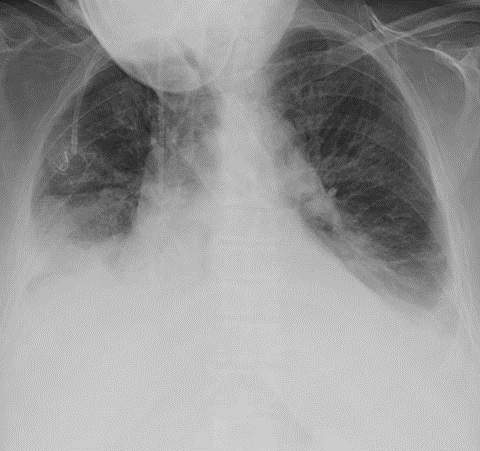
Figure 2. Portable chest x-ray taken just after admission to the ICU.
Which of the following are true? (Click on the correct answer to proceed to the second of four panels)
- The EKG shows atrial fibrillation with a rapid ventricular response
- She should be immediately intubated for airway protection
- The chest x-ray shows bilateral pleural effusions
- 1 and 3
- All of the above
Reference as: Loftsgard T, Frost A, Evans D, Kolbet K. April 2015 critical care case of the month: half-sided light house. Southwest J Pulm Crit Care. 2015;10(4):159-70. doi: http://dx.doi.org/10.13175/swjpcc031-15 PDF