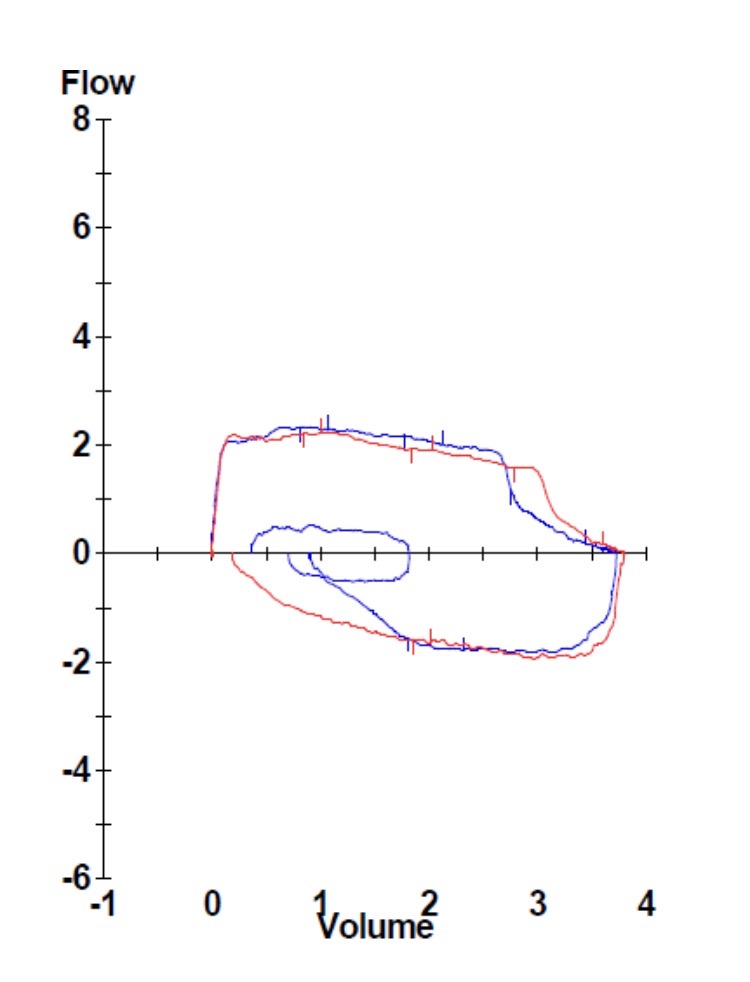
Figure 1. Flow-loop demonstrating fixed large airway obstruction.

Figure 2. Subglottic stenosis.
A 40 year-old previously healthy woman presented with a three-month history of exercise-induced shortness of breath. Clinical exam revealed inspiratory stridor. Spirometry was remarkable for flattening of the inspiratory and expiratory limbs of the flow-volume loop (Figure 1). Fiberoptic bronchoscopy revealed subglottic tracheal stenosis (Figure 2). The patient subsequently underwent successful balloon dilation of the involved segment and has remained symptom free.
Tracheal stenosis may be related to previous airway trauma, collagen vascular disease, sarcoidosis, or vasculitis. The clinical presentation is characterized by exertional dyspnea with stridor. The flow-volume loop classically demonstrates a pattern of fixed upper airway obstruction, with flattening of both the inspiratory and expiratory limbs of the curve. CAT scanning is usually supportive of the diagnosis, and bronchoscopy is confirmatory. In the absence of an identifiable etiology, the condition is termed idiopathic tracheal stenosis. Idiopathic subglottic stenosis is a subgroup of tracheal stenosis that occurs in young women, and that is limited to the first two rings of the proximal trachea (1). Bronchoscopic tools, including balloon dilation, laser, and electrocautery have all been used with safety and efficacy for the treatment of idiopathic subglottic stenosis (2).
Charles J. Van Hook MD and Britt Warner PA
Longmont United Hospital
Longmont, CO USA
References
- Nussbaumer-Ochsner Y, Thurnheer R. Images in clinical medicine: subglottic stenosis. N Engl J Med. 2015 Jul 2;373(1):73. [CrossRef] [PubMed]
- Solly WR, O'Connell RJ, Lee HJ, Sterman DH, Haas AR. Diagnosis of idiopathic tracheal stenosis and treatment with papillotome electrocautery and balloon bronchoplasty. Respir Care. 2011 Oct;56(10):1617-20. [CrossRef] [PubMed]
Cite as: Van Hook CJ, Warner B. Medical image of the week: idiopathic subglottic stenosis. Southwest J Pulm Crit Care. 2017;15(1):39-40. doi: https://doi.org/10.13175/swjpcc076-17 PDF