Lewis Wesselius MD
Department of Pulmonary Medicine
Mayo Clinic Arizona
Scottsdale, AZ
History of Present Illness
A 56 year old woman with a history of rheumatoid arthritis (RA) for 26 years was seen as an outpatient. She has a recent history of increased cough, sputum and dyspnea.
PMH, FH, SH
She was originally from India but had lived in Singapore from 2011 to June 2013 before moving to Phoenix. In 2009, she was diagnosed with Mycobacterium avium-intracellulare (MAI) on bronchoscopy and started on azithromycin, ethambutol, and rifabutin. She was unable to tolerate rifabutin but was continued on ethambutol and azithromycin. She had been on etanercept for her RA which was held after the diagnosis of MAI. She had negative sputum cultures for MAI in September 2012 and her ethambutol and azithromycin were stopped. In May 2013 she had increased symptoms and bronchoscopy demonstrated Pseudomonas and nontuberculous mycobacterium (NTM). She was treated with cefipime/ciprofloxacin for 6 weeks prior to moving to Phoenix.
She does not smoke or drink. Her FH is noncontributory.
Medications
- Celecoxib 200 mg bid
- Gabapentin 600 bid
- Methotrexate 15 mg weekly
- Prednisone 5 mg daily
- Tramadol 50 mg every 4 hours prn
Physical Examination
Afebrile. SpO2 96% on room air.
Chest: scattered crackles in both lungs, no wheezes.
There were joint deformities typical of chronic RA, but otherwise the remainder of the physical exam was unremarkable.
Radiology
She brings a CT scan from 2009 (Figure 1).
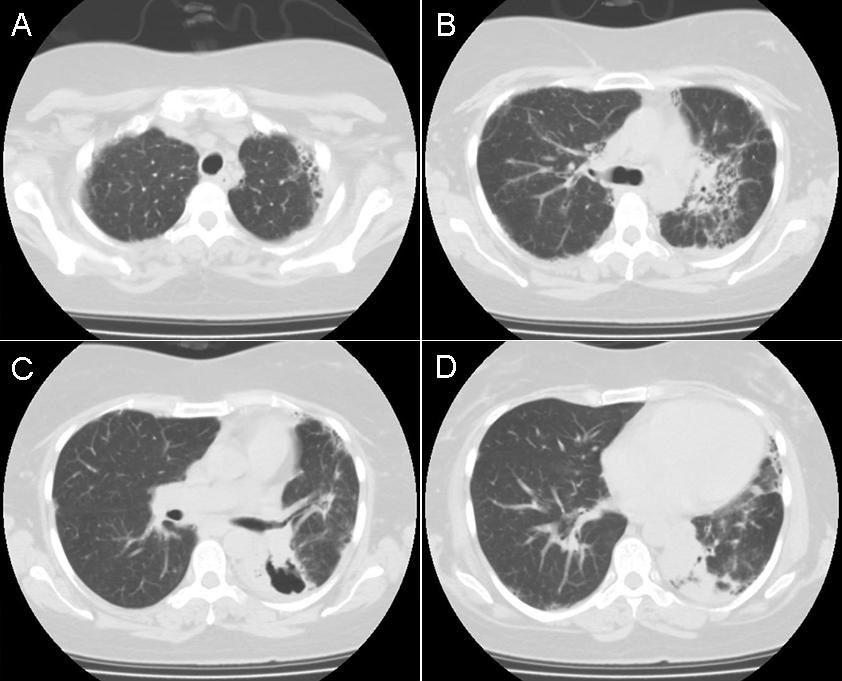
Figure 1. Panels A-D: Representative static axial lung images from a thoracic CT scan performed in 2009. Lower panel: movie of selected lung images from the thoracic CT scan performed in 2009.
What should be done next? (Click on correct answer to move to next panel)
Reference as: Wesselius LJ. February 2014 pulmonary case of the month: faster is not always better. Southwest J Pulm Crit Care. 2014:8(2):74-8. doi: http://dx.doi.org/10.13175/swjpcc168-13 PDF