John N. Galgiani, MD
Valley Fever Center For Excellence
The University of Arizona
Tucson, AZ
Preface
In the south and central deserts of Arizona and the central valley of California, Valley Fever should be a familiar phrase to clinicians and patients alike. It is estimated that over 50,000 persons each year, or approximately 1% of the population within the most endemic regions, seek medical care for newly acquired Valley Fever infections. Certain medical and surgical specialists practicing in these areas are particularly likely to be aware of the less frequent but more serious complications of the disease. In recent years, both the Centers for Disease Control and Prevention and the Arizona Department of Health Services have contributed significantly to our understanding of Valley Fever as a public health problem.
However, despite the significant impact of these complications on regional public health and individual lives, the majority of these infections are managed by primary care clinicians either without an accurate diagnosis or with sub-optimal care.
In January 1996, the Valley Fever Center for Excellence established a hotline that physicians and others with questions about Valley Fever could call for information. From the questions received through the hotline, it became increasingly apparent that many details about the causes of and necessary responses to Valley Fever were not fully understood.
One area of particular importance was the need for timely diagnosis and proper management of the initial respiratory infection. Early diagnosis of Valley Fever by primary care professionals can improve patient care by reducing patient anxiety, unneeded diagnostic tests, and unwarranted use of antibacterial agents. Moreover, early appropriate treatment can reduce the incidence of serious complications requiring additional treatment. We hope to improve this situation with this revised edition of Valley Fever (Coccidioidomycosis) Tutorial for Primary Care Professionals.
The purposes of this monograph are two-fold. First, it is intended to be a syllabus to accompany a medical education program on the primary care aspects of coccidioidomycosis organized by the Valley Fever Center for Excellence. Slide presentations from the CME program can be found at the Valley Fever Center for Excellence website (www.vfce.arizona.edu). While this syllabus does not follow the presentation structure of the CME program, it covers much of the same information.
Medical centers, health maintenance organizations, or other medical groups interested in bringing this program to their site for their clinicians can arrange to do so by contacting the Center at (520) 626-6517 or through its website at http://www.vfce.arizona.edu.
Second, this publication is designed to be a reference for the office shelf. The information it contains is not intended to be an exhaustive review of the disease. The content was selected for its relevance and usefulness to busy family practitioners, internists, emergency room personnel, and others dealing with patients in the primary care setting, especially within regions endemic for the Coccidioides species.
We hope you find this information helpful. Formatting and printing of this version of Valley Fever (Coccidioidomycosis) Tutorial for Primary Care Professionals was made possible by an unrestricted grant to the Valley Fever Center for Excellence from Nielsen BioSciences, whose support we greatly appreciate.
Overview of Coccidioidomycosis
History
The first patient recognized with what is now known as coccidioidomycosis was an Argentinean soldier in 1893. The first North American patient was recognized by a San Francisco surgeon the following year. First thought to be a protozoan infection, its true fungal nature was determined in 1900.
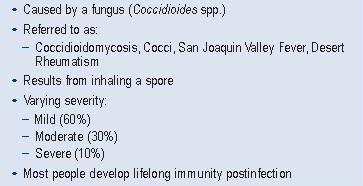
Initially, the infection was considered rare and fatal, but that understanding has changed dramatically. By 1935, it had been linked to the common illness known as San Joaquin Valley Fever and by the 1940s, its existence within southern Arizona was well appreciated. In addition, it is now recognized to present in a range of severities, and most people that contract the disease are known to become immune to it after a single infection (Table 1).
Table 1. Valley Fever at a Glance
Mycology
The fungal species that cause Valley Fever are in the genus Coccidioides: C. immitis and C. posadasii. In the past, all strains were designated as C. immitis, but recent genetic analysis has shown that strains segregate into two distinct groups. Strains now designated C. immitis in most cases originate from infections contracted in California. Those designated C. posadasii are from infections contracted elsewhere. At the present time, most clinical laboratories do not determine species for new isolates. Therefore, the simple case designation Coccidioides spp. is technically accurate.
In the soil (Figure 1), Coccidioides spp. survive as mycelia, growing beneath the surface at a depth ranging from inches to a few feet.
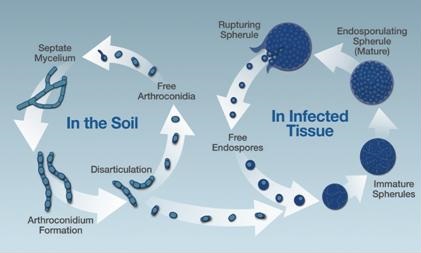
Figure 1. The life cycle of Coccidioides spp.
Since the fungus is an obligate aerobe, oxygen content is a major factor limiting the depth that it can survive in the dirt. During rainy periods, mycelia proliferate and grow closer to the surface. When the rains cease and the ground dries, the mycelia stop elongating. Along their length, alternating cells undergo autolysis, lose their internal contents, and their walls become extremely brittle. The remaining barrel-shaped single cells (known as arthroconidia) are then easily disrupted.
The size of each arthroconidium is approximately 3-5 μm. This is small enough to both remain suspended in the air and be inhaled deep into the lungs, thereby establishing an infection. At that point, an arthroconidium transforms into a spherical shape and enlarges, frequently to as much as 75 μm in diameter. Inside the growing spherule, the cell wall invaginates to repeatedly transect the space, dividing into many scores of subcompartments, each containing viable cells, termed endospores. In active infections, a mature spherule ruptures its outer wall and releases the endospore progeny, each of which can develop into another spherule. If specimens containing spherules are cultured in a laboratory, growth reverts to the mycelial form.
Epidemiology
The endemic regions of Coccidioides spp. roughly correspond to the “lower Sonoran life zone” and are areas of low rainfall, high summer temperatures, and moderate winter temperatures. Regions that fit that description are found in the
southern deserts of Arizona (including Maricopa, Pinal, and Pima counties), the central valley and southern portions of California (including Kern, Tulare, and San Luis Obispo counties), the southern tip of Nevada, southern Utah, southern New Mexico, western Texas (especially along the Rio Grande), and the northern and Pacific coastal areas of Mexico. Recently, a pocket of Coccidioides has been identified in Washington State. Some areas have been identified in Central and South America as well (Figure 2).

Figure 2. Shaded areas indicate suspected coccidioidomycosis distribution in the Western Hemisphere.
Even within endemic regions, the distribution in the soil is not uniform, and, in fact, most acreage appears free of the fungus. Thus, while occasionally disruption of soil produces increased risk of exposure, such activity often does not. Conversely, windy conditions, which typically involve large areas of the desert, may more likely result in arthroconidia becoming airborne and distributed across urban and rural areas alike. The implication is that exposure to Coccidioides spp. is more associated with living in or visiting endemic areas per se than it is with engaging in activities associated with heavy dust exposure.
Since infection occurs after inhaling an arthroconidium that has developed in the soil, virtually all infections originate in an endemic region. Very rarely, dirt which contains arthroconidia carried from the endemic region has been the source of infection elsewhere. It’s important to note that infection resulting from respiratory exposure to an infected patient has never been reported, and patients with Valley Fever need not be isolated from others. Peak infection rates occur during the driest periods of the year. In Arizona, this is the early summer and late fall, whereas in California, it is all throughout the summer.
Spectrum of Disease
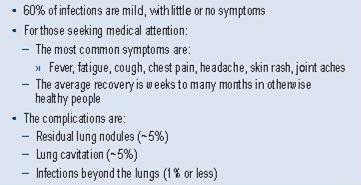
The majority of infected persons have symptoms so mild that they see no need for medical attention. Of the approximately one-third of infected persons who do suffer a clinical illness, the symptoms are primarily those suggesting community-acquired pneumonia. For most such patients, it is not possible without specific laboratory testing to distinguish Valley Fever pneumonia from that caused by other etiological agents.
Whether diagnosed or not, most infections are controlled by induction of immunity, although the associated illness may last for many weeks to many months. Approximately 5% to 10% of infections result in pulmonary sequelae, and 1% or less result in the spread of the infection outside of the lungs. This leads to destructive lesions in the skin, bones, joints, meninges, and virtually any other organ or tissue in the body to which the infection has spread. These complications produce a large amount of chronic morbidity and cause an average of fewer than 200 deaths annually in the United States (Table 2).
Table 2. Spectrum of Coccidioidomycosis
Current Therapies
Many patients with Valley Fever pneumonia require no treatment, and the illness resolves as a consequence of acquired immunity. However, in some patients, coccidioidal pneumonia is acute and very severe. In others, it produces various progressive pulmonary syndromes or leads to spread of infection to other parts of the body. Such complications dictate the need for treatment, and even so the infection may remain difficult to control.
A majority of complicated infections follow a subacute or chronic progression, and initial therapy usually involves oral administration of azole antifungals, such as fluconazole or itraconazole. Typically, treatment is continued for many months to years. When therapy is discontinued after the apparent successful control of disease, a relapse of infection occurs in approximately one-third of patients.
Therefore, some patients may need lifelong therapy to maintain control. Chief among these are patients with deficiencies in cellular immunity or those with coccidioidal meningitis. Amphotericin B is effective only if administered parenterally, and its use is often associated with significant side effects and toxicities. Despite these drawbacks, in rapidly progressive infections, amphotericin B remains the preferred initial treatment.
The Importance of Valley Fever in Primary Care
Case Reporting
Coccidioidomycosis is a reportable disease at the national level, and reporting is required in Arizona and California where cases annually number in the thousands (Figure 3).
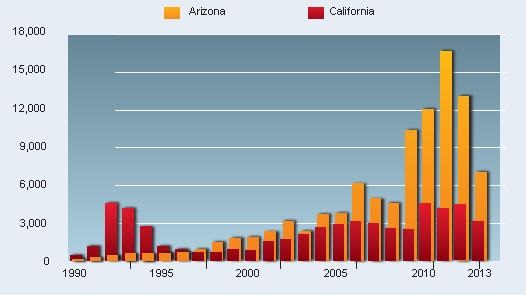
Figure 3. Annual number of cases of coccidioidomycosis reported in Arizona and California.
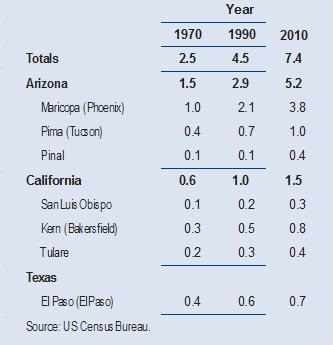
In addition, the fact that Arizona has approximately twice as many infections as California is related to the differences in the population sizes in the most intensely endemic regions of the two states (Table 3).
Table 3. Population (in millions) of Selected Counties in Regions Highly Endemic for Coccidioidomycosis.
In 2007, the Arizona Department of Health Services conducted a telephone survey of nearly 500 persons, approximately 10% of those reported being newly diagnosed with Valley Fever that year (1). From these interviews, it was found that more than half were ill for longer than six months, 75% were unable to do usual daily activities for longer than three months, and 75% of workers missed an average of one month of employment. Also found were significant delays in diagnosis.
For example, patients waited 44 days before seeking care for their illness. Once care was sought, there was an additional average delay of five months involving three or more clinic visits before the correct diagnosis was made. The impact on the health care system was substantial since over half of patients sought their care from emergency rooms, 40% of those were hospitalized one or more nights, and 25% of the patients required 10 or more visits to clinicians to manage their illness. From Arizona hospital records, there were over 1700 admissions resulting from Valley Fever infections in 2012, costing over $100 million.
As significant as these findings are, other analyses indicate that compared with the number of reported infections, the number of undiagnosed infections is even more substantial. In one study conducted in Phoenix, only 2% to 13% of patients with community-acquired pneumonia were tested for Valley Fever (2). In contrast, when Tucson patients with a clinical diagnosis of community-acquired pneumonia were prospectively tested for Valley Fever, 29% were found to be positive (3).
These and other less direct measurements all indicate that approximately 50,000 patients annually seek medical care for Valley Fever pneumonia (4). Since most coccidioidal infections can only be diagnosed by specific laboratory testing, the lack of clinicians testing for Valley Fever could easily account for the under-reporting of illness by as much as 90%.
Undiagnosed infections are almost certainly not as serious as those that are recognized. Nonetheless, there are several very important reasons why diagnosis, especially in the primary care setting, should be pursued.
Value of Early Diagnosis
A primary reason for diagnosing early coccidioidal infections is simply that it provides patients with answers to why they are feeling so poorly. By giving an illness a specific name, it removes the patient’s fear of the unknown. Diagnosis has always been a major contribution by clinicians, and the value of diagnosis to patient satisfaction should not be underestimated.
This is especially true for older patients, where the concern exists that an undiagnosed respiratory illness may represent cancer. A myriad of physical, mental, and emotional consequences are associated with an incorrect or suspected diagnosis of cancer.
For patients of all ages, an accurate diagnosis allows for reassurance in most cases and appropriate prognostic patient education.
In addition, early diagnosis of Valley Fever reduces or eliminates the need to search for another diagnosis. The symptoms associated with Valley Fever that take weeks or even months to resolve often prompt concerned clinicians to subject their patients to diagnostic blood tests, chest X-rays, CT scans, PET scans, bronchoscopy, percutaneous fine-needle aspiration, and even thoracotomies. These procedures have attendant costs, discomfort, and potential complications, which might be avoided if coccidioidomycosis were known to have been responsible for the symptoms that patients experience.
A third benefit of diagnosing coccidioidal infections early is the reduction or elimination of empiric therapy for bacterial infection. Patients with persistent respiratory complaints often receive empiric antibiotics in an ambulatory practice.
In one study, 81% of patients with Valley Fever pneumonia received at least one course, and 31% received multiple courses of antibacterial treatment for their illness (3).
In addition to the cost of antibiotics, this strategy has the potential to cause adverse events for the patient and increase antibiotic resistance in the community. A less frequent but potentially more serious problem is the use of corticosteroids for the cutaneous or rheumatologic complaints that may accompany primary coccidioidal infection. The anti-inflammatory effects of corticosteroids may impede host defenses, and their use in patients with early coccidioidal infections may cause adverse effects.
Finally, by establishing a diagnosis of coccidioidomycosis early, complications (should they arise) may be more quickly recognized and treated. Complications of coccidioidal infection usually manifest within months of the initial infection.
For this reason, symptoms that are associated with or develop in the weeks following a new coccidioidal infection may indicate extrapulmonary spread. A more detailed evaluation of new symptoms at this stage may identify a need for treatment earlier and reduce tissue destruction and consequent morbidity (Table 4).
Table 4. The Value of Early Diagnosis
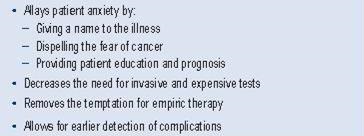
In summary, the attitude that primary care professionals take regarding early diagnosis of coccidioidal infections is critical to all further discussion about the proper management of this infection in the primary care setting. Historically, the approach in general has been passive, leaving diagnosis and treatment to only the most severely ill. Providing an accurate, early diagnosis can decrease patient anxiety and eliminate unwarranted diagnostic testing and unnecessary exposure to antibiotics. Also, it can allow for earlier identification and treatment of complications.
The Arizona Department of Health Services has recommended that physicians whose patients have endemic exposure to Valley Fever be tested for this possibility should they develop signs and symptoms of pneumonia. The Valley Fever Center for Excellence endorses that recommendation as reflected in this monograph. The following section, then, describes general strategies for primary care professionals to identify and manage this important disease.
Primary Care Management of Coccidioidomycosis
Overview
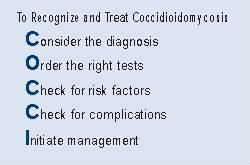
The following section outlines an approach for recognizing a new infection, assessing its impact on the patient, and subsequently managing the illness depending upon its level of complications. We have developed an acronym (COCCI) for this approach based on 5 important steps.
Spectrum of Clinical Manifestations of Valley Fever
Consider the Diagnosis
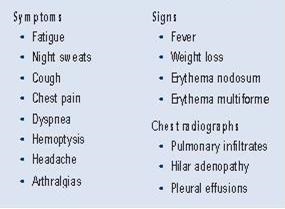
The incubation period of coccidioidal infection ranges from 7 to 21 days, after which a variety of manifestations develop. The most common symptoms are fatigue, night sweats, and pulmonary symptoms (cough, chest pain, dyspnea, and hemoptysis). Although difficult to quantify, fatigue is often the most prominent symptom. Stories like “I went to bed and didn’t wake up for 15 hours” or “I got up for breakfast and then was exhausted” are common.
When a cough is present, it frequently is not particularly productive of large amounts of sputum. Fever is present in nearly half of patients. A headache occurs in approximately one-fifth of the patients with early infection; fortunately, as a transient symptom, this does not represent meningitis. Weight loss of as much as 5% to 10% is also common with coccidioidal infections. It is apparent from this that the clinical presentation overlaps substantially with the presentation of many other types of respiratory illnesses.
Skin manifestations include a diffuse nonpruritic maculopapular eruption which has been noted to occur in 16% of males and 7% of females, especially children and young adults. It is so transient and seemingly inconsequential that it is often missed. More notable are erythema nodosum (seven to eight times more frequent in women than men) and erythema multiforme. These two rashes are not specific for coccidioidomycosis. However, when found in patients with endemic exposure to Coccidioides spp., Valley Fever is frequently responsible.
Another symptom is diffuse and migratory arthralgia, present in 22% of patients. Joints may be mildly inflamed and painful but typically do not exhibit an effusion. The triad of fever, erythema nodosum, and diffuse arthralgias has produced the synonym of “desert rheumatism” for the disease. All of these manifestations are thought to be immunologically mediated and not the consequence of viable fungal cells in either the skin or the joints.
Chest radiographs often, but not always, disclose abnormalities associated with the early infection. Pulmonary infiltrates are usually one-sided and are typically patchy and not as consolidated as seen with bacterial infections. Often there is associated ipsilateral hilar adenopathy. Peripneumonic pleural effusions may also occur as part of a primary infection. Although disease of one lung is the rule, the process can occasionally be bilateral (Table 5).
Table 5. The Clinical Manifestations of Valley Fever
Routine laboratory findings commonly do not show specific abnormalities. Peripheral blood leukocyte counts are usually normal or only slightly elevated. Eosinophilia is sometimes present and occasionally to strikingly high levels. Erythrocyte sedimentation rate and C-reactive protein are often elevated.
However, recent studies indicate that serum procalcitonin levels are usually normal, which may be a useful way to distinguish coccidioidal from bacterial pneumonia.
Attempts to use clinical presentation and routine laboratory results as an indicator of coccidioidal infection have been uniformly unsuccessful. In one study, several patient findings were significantly associated with coccidioidal infection, as compared to patients with other causes of acute respiratory problems (5). However, the predictive value of these abnormalities was very limited and not of practical help in identifying most infections.
Selecting Patients for Evaluation
Since the signs, symptoms, and routine laboratory abnormalities are nonspecific, virtually any patient evaluated for a variety of complaints, especially those related to the respiratory system, could arguably be evaluated for coccidioidomycosis. The more patients that are tested for Valley Fever, the more infections are likely to be diagnosed.
On the other hand, despite the prevalence of Valley Fever within the endemic patient population, many other acute illnesses also exist. Thus, by increasing provider sensitivity and the number of tests ordered to diagnose Valley Fever, the overall proportion of tests that are diagnostic will decrease.
A critical step for clinicians in a busy practice is to establish routine indications for ordering the appropriate tests. Several indications are proposed, which are selected for simplicity and application to common situations (Table 6).
Table 6. In patients who reside in or have traveled to endemic regions, consider testing for coccidioidomycosis if any of the following indications are present:
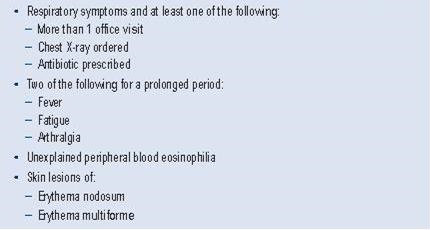
Order the Right Tests
Detection of Anticoccidioidal Antibodies in Serum: Serologic Tests
For diagnosing primary infections, serologic tests are the most commonly employed laboratory approach. Of the variety of tests available, some are highly specific for an active infection, while a few have a significant frequency of false- positive results.
Specific tests are typically selected by the director of the clinical laboratory. Factors involved in such selection include the cost and rapidity of obtaining results, the availability of tests from specific reference laboratories that provide other testing services, and the sensitivity and specificity of the tests. Moreover, tests available to a specific provider may change over time because of renegotiated contracts and other factors. This has complicated the interpretation of coccidioidal serologic testing. Because of this, the following two general principles are useful in the primary care setting:
First, in most circumstances, a positive serologic test for coccidioidal antibodies is highly presumptive of a current coccidioidal infection. Therefore, a report of a positive serologic test should always be reviewed by someone familiar with test interpretation. Second, a negative serologic test never excludes the presence of a coccidioidal infection. For this reason, in evaluating a possible coccidioidal infection, one or even two repeated serologic tests will increase the sensitivity for diagnosis. If repeated testing over the course of two months fails to produce a serologic diagnosis, further serologic testing is likely to be unrewarding.
“A positive serologic test for coccidioidal antibodies is highly presumptive of a coccidioidal infection. Therefore, a positive serologic result should always be reviewed by someone familiar with test interpretation.”
“A negative serologic test should never exclude a coccidioidal infection. In evaluating a possible coccidioidal infection, repeated serologic tests will increase the sensitivity for diagnosis.”
Tube Precipitin (TP) Antibodies
Antibodies of this type were originally detected by the presence of a precipitin button that formed at the bottom of a test tube after overnight incubation of patient serum mixed with coccidioidal antigen. Because IgM is most adept at forming such immune precipitins and because these reactions were detected early after onset of infection, this test is now often referred to as the “IgM test.”
The antigen responsible for this reaction is a polysaccharide from the fungal cell wall. Up to 90% of patients will have TP antibodies detected at some time within the first three weeks of symptoms, and this will decline to less than 5% after seven months of the onset of a self-limited illness.
Complement Fixing (CF) Antibodies
When patient serum is mixed with coccidioidal antigen, an immune complex forms which consumes complement. This event is detected by the subsequent addition of tanned red blood cells, which normally lyse in the presence of complement but remain intact if the complement is depleted. Since IgG is the immunoglobulin class usually involved in such immune complexes, this test is often referred to as the “IgG test.”
Although this test was originally developed using various complex extracts of C. immitis, it is now known that the antigen involved in this reaction is a chitinase, a protein enzyme important in the structure of the fungal cell wall. In early coccidioidal infections, CF antibodies are detected somewhat later and for longer periods than TP antibodies. CF antibodies can be detected in other body fluids and their detection in the cerebrospinal fluid is an especially important aid to the diagnosis of coccidioidal meningitis.
Another difference between CF and TP antibodies is that CF results are expressed as titers, such as 1:4 or 1:64, indicating the greatest dilution of serum at which complement consumption is still detected. In general, higher CF titers reflect more extensive coccidioidal infection, and rising CF antibody concentrations are associated with worsening disease. Thus, serial determinations of CF antibody concentrations are of prognostic as well as diagnostic value.
Immunodiffusion Tests (IDTP, IDCF)
Antibodies that were detected by the original TP or CF tests can be detected by an alternative procedure known as the immunodiffusion (ID) tests (IDTP and IDCF, respectively). Although the conduct of the IDTP and IDCF tests is quite similar, each uses a different antigen to measure different types of antibodies.
As with the original tests, the IDTP is reported by some laboratories as the “IgM test” and the IDCF as the “IgG test” result. Both tests have been found to be at least as sensitive as their original counterparts. Moreover, immunodiffusion tests are amenable to being manufactured and distributed as commercially prepared kits, thus allowing the tests to be performed in labs not fully dedicated to a mycology specialty.
Enzyme-linked Immunoassays (EIA)
An EIA test for coccidioidal antibodies is available commercially. The test kit allows for the specific detection for IgM or IgG antibodies. However, these results are not interchangeable with IgM or IgG test results. Positive EIA results are highly sensitive for coccidioidal infection. However, false-positive results have been noted with the IgM EIA test. How frequently this occurs is not a settled issue (6-8).
Latex Tests
Latex tests for coccidioidal antibodies are also commercially available. They are attractive to clinical laboratories because of their ease of use and rapidity of obtaining a result. However, there are significant numbers of false-positive reactions, and therefore a positive latex test is not as reliable as any of the other tests described in this section.
Cultures for Coccidioides spp.
Isolating Coccidioides spp. from sputum or another clinical specimen is definitive evidence of a coccidioidal infection. Despite this, early infections are usually not diagnosed by culture. The reasons why cultures are not routinely obtained in the ambulatory care setting are related to several factors.
First, fungal cultures are an unusual request in the ambulatory care setting. Although it would be valuable if this were to change, requesting fungal cultures on a sputum specimen currently may be disruptive to workflow. Another consideration is that patients with coccidioidal pneumonia may not be able to produce a specimen for culture. While this problem can usually be circumvented, it takes extra steps. Finally, there is a potential risk to laboratory personnel of isolating Coccidioides spp.
Laboratories handling fungal cultures should be thoroughly versed in safe- handling of such specimens and culture medium, and small outpatient laboratories may not be so equipped or trained. None of these considerations are absolute barriers to obtaining culture confirmation. Since negative serologies do not exclude the diagnosis of coccidioidomycosis, cultures may be the only way to obtain a timely diagnosis in some patients. As a general rule, the more serious the illness, the more likely fungal cultures should be considered as an essential part of the diagnostic evaluation.
Handling of Specimens
Sputum or other clinical specimens should be collected in a sterile container. This may be done in the clinic at no risk to personnel, since the infection is not transmitted from the primary specimen. Patients with scant sputum can be asked to take a specimen cup home with them and collect a specimen early in the morning (when sputum is usually more readily retrievable) and then return the cup.
Such specimens can be stored refrigerated until transfer to the medical facility. For more serious problems, other respiratory secretions (bronchoscopic aspirates) and tissue specimens (skin or bone biopsies) can be submitted for culture.
Laboratory Evaluation
Direct examination of secretions can be performed immediately or after the addition of potassium hydroxide. Although culture results are more sensitive than direct examination, identification of spherules in this way is diagnostic and very rapid. Coccidioides spp. cannot be detected by Gram staining. However, spherules can be seen with cytology stains such as are performed on bronchoscopy specimens, by hematoxylin and eosin stains of tissue sections, and with other specialized stains.
Coccidioides spp. are not particularly fastidious and grow well on most mycologic and bacteriologic media. Furthermore, growth usually develops within four to seven days of incubation. Some clinical laboratories within the coccidioidal endemic region have used these characteristics to advantage by holding all routine bacteriologic sputum cultures for a week before discarding the plates, since some patients who are thought to have bacterial pneumonia will actually yield Coccidioides spp.
When growth occurs, it is typically as a white (nonpigmented) mold. However, there are many exceptions to this general appearance, and the morphologic appearance is not reliable in determining if the fungus is or is not Coccidioides spp.
Once growth is evident on culture medium, care should be taken not to open the culture container except in an appropriate biocontainment cabinet. Cultures at this stage are infectious and can cause disease in persons exposed to them unless the cultures are properly handled. Since the morphologic appearance of Coccidioides spp. is not sufficient to determine the species, additional laboratory testing must be carried out for specific identification.
The most common way for microbiologists to perform additional testing is to detect a specific DNA sequence using a commercially available DNA probe. Smaller laboratories often refer the culture to a reference laboratory where species identification is completed.
As of December 2012, Coccidioides spp. are no longer designated select agents by the Centers for Disease Control and Prevention (CDC).
Skin Testing
Dermal hypersensitivity to coccidioidal antigens is highly specific for past coccidioidal infection, and if used in patients when they are healthy, it can index patients as to whether they are at risk of future illness due to Valley Fever.
For example, persons who demonstrate a reactive skin test are very likely to be immune for life and have little chance of future coccidioidal problems. On the other hand, for those who do not react, Valley Fever remains a possible etiology in a future illness. However, because skin test results remain positive after infection in most persons for life, it may not relate to the current illness. In addition, some of the most serious infections may be associated with selective anergy, and the skin test may not demonstrate reactivity.
Therefore, as useful as skin test results are for indexing risk in patients while healthy, important limitations exist when used as a screening procedure for recent or current infection. If Valley Fever is diagnosed by other means, skin testing may have prognostic significance, as patients with progressive infections often fail to develop dermal reactivity to coccidioidal antigens. Since the 1990s, there was no coccidioidal skin test commercially available. However, a company (Nielsen BioSciences, San Diego, CA) has redeveloped a spherule-based skin test antigen (SPHERUSOL®) and has received approval from the FDA to market it.
Results of a skin test are measured at 48 hours after the antigen is injected intradermally. Induration of greater than 5 mm is considered reactive. Erythema at the injection site is not of diagnostic value. Coccidioidal skin testing does not influence coccidioidal serology results.
Check for Risk Factors
The First Step Postdiagnosis
Once a diagnosis of coccidioidal infection is established, the next step is to review any possible risk factors that might make the patient particularly susceptible to complications. This is usually accomplished during a complete history and physical examination.
Immunosuppression
By far the most clearly demonstrable risk of complications from a coccidioidal infection is the coexistence of major immunosuppressive conditions that adversely affect cellular immunity. These would include immunosuppression to prevent rejection of organ transplants, AIDS in HIV-infected persons, and anti–tumor necrosis factor therapy for rheumatologic conditions. For example, the risk of infections extending beyond the lungs in renal transplant recipients can be as high as 75%. This risk is much greater than the risk of a similar complication in the general population.
Immunosuppressive conditions that affect humoral immunity appear to have relatively little risk for complications of coccidioidal infection. Similarly, splenectomy, hypocomplementemia, or neutrophil dysfunction syndromes are not major risk factors for this disease.
Diabetes Mellitus
Patients with diabetes appear to have an increased risk of pulmonary complications (9). While many of such patients resolve their initial infection without residual problems, a disproportionate number seem to develop symptoms related to pulmonary cavities and chronic pneumonia. There is little or no evidence that this group of patients is at increased risk for developing extrapulmonary infections.
Pregnancy
Women who contract Valley Fever during pregnancy are at particular risk of serious infection. Those at highest risk for serious infection are women diagnosed during the third trimester or immediately postpartum. Such infections may be life-threatening and should be regarded as complicated management problems.
Other Risk Factors
There are additional factors that should be considered relevant to the risk of complications from coccidioidal infection. Complications are more frequent in men than in women and in adults than in children. Life-threatening infections are more common in the elderly. Recent evidence suggests this is related in part to accumulated comorbidities in aging persons rather than age itself (10).
In addition, there appears to be an increased risk of disseminated infection among African Americans, Filipinos, and perhaps other racial groups. Racial predilection for complications is somewhat conjectural since the exact definitions of racial groups are in dispute and carefully controlled epidemiologic studies are not available. Even if racial differences exist (as most authorities believe), the increase in risk may be only four-fold above that of the population as a whole.
Check for Progressive Pulmonary Syndromes or Disseminated Disease
Assessing Complications
Even in the absence of the risk factors previously discussed, it is important to assess patients with coccidioidal infections for complications because they can also occur in patients without apparent reason.
Complications from initial coccidioidal infections are divided into those that occur in the chest and those that involve parts of the body outside of the lungs (extrapulmonary dissemination). These two types of complications usually do not overlap. Most complications produce localized symptoms and signs of chronic or subacute inflammation. As a result, a careful review of symptoms and physical examination are usually a sufficiently sensitive initial screen.
Most complications manifest within the first year or two after the initial infection. If a new complaint develops in association with a recent coccidioidal infection, its possible relationship to the infection should be considered. For example, in general practice, low back pain is a common symptom, and mild discomfort is often managed symptomatically before extensive diagnostic studies are undertaken.
However, if this symptom were to occur in a patient within weeks or months of developing coccidioidal pneumonia, it may be useful to recommend a radionuclide scan to determine if the new symptom is due to infection in the lumbar vertebrae. This is done to detect complications early, before serious tissue destruction occurs. Similarly, persistent or progressive headaches, skin lesions, or joint effusions in the context of a recently diagnosed coccidioidal pneumonia might warrant more detailed investigation with lumbar puncture, biopsy, or aspiration, respectively.
Persistent or Slowly Resolving Pneumonia
Most pulmonary infections are subacute in nature. Without treatment, symptoms usually improve within the first month but may not completely resolve for several months. In some patients, the course of illness is even more protracted. There is no consensus regarding how protracted illness must be before it is considered as slowly resolving. However, in studies of new therapies for coccidioidomycosis, entry criteria often specify that pulmonary disease must have been present for at least three months. In clinical practice, shorter periods of illness may be more reasonable.
Pulmonary Cavitation
Cavities form in approximately 5% of patients with coccidioidal pneumonia. Half of these cavities will disappear within the first two years. Many cavities cause no symptoms. Others cause discomfort, cough, hemoptysis, and occasionally constitutional symptoms of fatigue, night sweats, and weight loss. Occasionally, a coccidioidal cavity will rupture into the pleural space. This usually has an abrupt onset and consequently leads to prompt evaluation. Given the peripheral nature of many coccidioidal cavities, this event is surprisingly uncommon.
Chronic Fibrocavitary Pneumonia
A few patients experience repeated development of pneumonia over a period of many years. Sometimes, this includes different lobes of the lung.
Diffuse Fulminant Pneumonia
In some patients, coccidioidal pneumonia is very severe, causing hypoxia and requiring respiratory support to prevent respiratory collapse. This is obviously a major complication and is handled very differently than most infections.
Extrapulmonary Dissemination
When infection spreads beyond the lungs, it usually does so within the first several months after the initial infection and nearly always within the first two years. In this way, coccidioidal infections differ from tuberculosis, which commonly returns decades after the initial infection. An important exception to this rule is in the intervening development of major degrees of immunosuppression of the nature discussed previously. The most common sites of dissemination are skin, joints, bones, and the meninges. However, virtually any part of the body can be affected.
Initiate Management
Strategies for Uncomplicated Early Infections
Once a diagnosis of coccidioidal infection is established and a thorough evaluation for enhanced risk and evidence of complications has been accomplished, a rational management strategy can be formulated.
Patients who do not have risk factors, symptoms, or physical findings suggestive of progressive infection can be classified as having early uncomplicated infections. In general, a majority of patients will fall into this category and might be safely managed by primary care practitioners. The remainder may benefit from consultation with a specialist in infectious diseases, pulmonary diseases, neurology, or other disciplines to aid in developing a treatment plan. Management of complicated coccidioidal infections is beyond the scope of this monograph, but comprehensive treatment guidelines are available.
General guidelines for managing patients with uncomplicated infections are outlined in Figure 4.
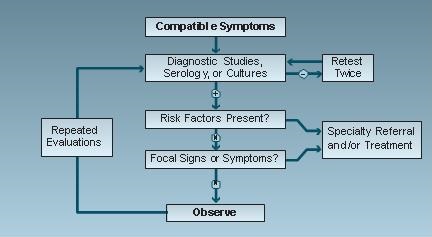
Figure 4. Managing uncomplicated coccidioidomycosis.
Health Education and Recommendations to the Patient and Family
Very commonly, establishing a diagnosis will be of great help to the patient because it clearly identifies the nature of the illness and allows the health care provider the opportunity to explain what may happen in the future. A general review of how patients contract Valley Fever, the typical symptoms, the need for therapy, or the lack of the need for therapy, may be helpful to put the patient’s experience in a more general and knowledgeable context.
Patient information leaflets have been prepared to facilitate this process and are available from the Valley Fever Center for Excellence.
Explaining that the illness usually improves slowly over a period of weeks to even months will be useful in allowing patients to align their expectations with the natural history of the illness. The patient can be advised that he or she cannot transmit the infection to others and therefore poses no risk to others.
Although the prognosis is generally favorable for most patients, it is important to explain to patients some of the infrequent but possible complications, both pulmonary and extrapulmonary. Worsening respiratory symptoms should prompt reevaluation, and new focal symptoms outside of the chest should be noted and, if they persist, be brought to the attention of the treating clinician. Explaining the need for follow-up to the patient even as the infection resolves without therapy should improve adherence to follow-up care.
Frequency of Follow-Up Health Care Visits
Continued follow-up is, in fact, at the core of the management of uncomplicated coccidioidal infections. This is needed to confirm that the illness remains uncomplicated and that more specific interventions are not necessary.
In addition, residual pulmonary abnormalities may remain, which should be documented for future reference so that they are not unnecessarily reevaluated as a new problem years later. In rare instances, coccidioidal infections and lung neoplasms have coexisted, and this possibility should be considered during the follow-up period.
The interval between medical visits varies according to the severity of the symptoms and the course of infection up to the point of diagnosis. If symptoms are still worsening, follow-up visits or telephone contact might be appropriate within days to a week later, since continued worsening may prompt reevaluation and the initiation of antifungal therapy.
On the other hand, if there is clear evidence of improvement, then a return visit might be appropriate in two to four weeks. After the first two or three visits, the intervals between visits typically range from one to several months. By two years, an uncomplicated coccidioidal infection can be considered resolved.
Monitoring the Course of Infection
Several clinical and laboratory findings are helpful to assess the course of infection. Generally, systemic signs of fever, night sweats, and weight loss are the first to abate as a coccidioidal infection improves. The respiratory symptoms of chest pain, cough, and sputum production may be more protracted.
Not infrequently, fatigue and an inability to resume normal activities are some of the last symptoms to resolve. Since this is commonly a chronic process, patients may fail to see changes in these symptoms from day to day, and only when asked to compare their current state with one week or one month earlier do they become cognizant of improvements. Often, having the patient keep a journal with entries every other week is a helpful tool to document progress.
Laboratory tests can also be helpful in providing objective evidence of improvement. Erythrocyte sedimentation rate, often elevated with early coccidioidal infections, is an inexpensive measure of systemic inflammation and can be used to monitor progress. Typically, this would not be measured any more often than on a weekly basis. In addition, the CF or IDCF antibody concentration is expected to decrease as a coccidioidal infection resolves, and it is important to demonstrate this response. If these results do not normalize as expected, concern should be raised that complications may be developing and that further diagnostic studies may be in order. Repeated serologic testing should seldom be any more frequent than every two weeks and usually ranges from one to several months between tests.
A suggested plan for follow-up timing for review of systems (ROS), physical examination, coccidioidal CF tests, and chest radiographs is shown in Table 7.
Table 7. Suggested Plan for Follow-up Visits.
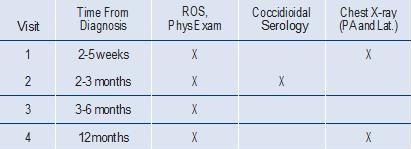
Chest radiographs should be repeated to demonstrate either resolution of all pulmonary abnormalities or to document what residual abnormalities persist. Early in the course of infection, the interval may be as frequent as several days until symptoms or radiographic findings demonstrate that abnormalities are stable or improving. Subsequent chest radiographs should be obtained either every several weeks or every several months. Often, two views of the chest are sufficient to monitor progress, and the increased sensitivity of CT scans is not usually needed as the patient improves.
Antifungal Therapy
For early uncomplicated coccidioidal infections, most patients can be managed without antifungal therapy. There are currently five commercially available oral antifungal drugs with activity for treating coccidioidal infections: ketoconazole, fluconazole, itraconazole, voriconazole, and posaconazole. Published reports have demonstrated activity of all of these agents in treatment of complicated coccidioidal infections, but there are no randomized trials demonstrating that any of these drugs shorten the course of early uncomplicated infections or prevent later complications. Two recent observational studies also provide no evidence for a beneficial effect in the pharmacologic treatment of early coccidioidal pneumonia (11,12).
Given this uncertainty, the decision whether to initiate antifungal drug therapy for uncomplicated coccidioidal pneumonia is highly individualized. This issue is addressed further in the Infectious Diseases Society of America (IDSA) Practice Guidelines (13). Treatment with fluconazole or itraconazole for such patients typically involves doses ranging from 200 to 400 mg per day, with treatment durations ranging from several to many months.
Treatment of complicated infections is beyond the scope of this monograph but is also addressed in the IDSA Practice Guidelines. The length of treatment for such patients ranges from one year to the entire course of the patient’s lifetime, depending upon the location of the infection and underlying risk factors.
The cost of therapy is substantial. Drug costs alone range from $2,000 to $20,000 per year, depending upon the specific drug and the daily dose prescribed.
Physical Therapy Reconditioning As an Approach to Persistent Fatigue
Not infrequently, patients who resolve all evidence of active infection continue to be disabled because of profound fatigue. For example, in a study from the University of Arizona that compared the impact of Valley Fever to mononucleosis, twice as many students with Valley Fever dropped out for a semester (14). It is very possible that this persistent symptom is a consequence of patients becoming deconditioned as a consequence of the fatigue that Valley Fever first produces.
If that is true, then referral to a physical therapist to assist the patient with a reconditioning program might be very helpful to hasten recovery. The Valley Fever Center for Excellence has initiated this practice, and the preliminary results have been encouraging.
Conclusion
Valley Fever represents a substantial public health problem, the true burden of which likely remains under-recognized. The clinical presentation of this disease is often non-specific, and increased awareness among clinicians, particularly those involved in primary care, about the disease is essential in order to ensure that patients with Valley Fever receive a timely and accurate diagnosis. Clinicians should maintain a high clinical suspicion for Valley Fever in patients who live in the endemic region or who have traveled to these areas. Although only a small proportion of patients with Valley Fever develop pulmonary complications or extrapulmonary disease, it is important to identify these complications as early as possible. For the other patients, most coccidioidal infections are uncomplicated. The five steps—Consider the diagnosis, Order the right tests, Check for risk factors, Check for complications, and Initiate management (COCCI)—are a simple way for generalists to identify those with complications and to manage uncomplicated infections without specialty referral.
References
- Tsang CA, Anderson SM, Imholte SB, et al. Enhanced surveillance of coccidioidomycosis, Arizona, USA, 2007-2008. Emerg Infect Dis. 2010;16(11):1738-44. [CrossRef] [PubMed]
- Chang DC, Anderson S, Wannemuehler K, et al. Testing for coccidioidomycosis among patients with community-acquired pneumonia. Emerg Infect Dis. 2008;14(7):1053-9. [CrossRef] [PubMed]
- Valdivia L, Nix D, Wright M, et al. Coccidioidomycosis as a common cause of community- acquired pneumonia. Emerg Infect Dis. 2006;12(6):958-62. [CrossRef] [PubMed]
- Campion JM, Gardner M, Galgiani JN. Coccidioidomycosis (Valley Fever) in older adults: an increasing problem. Ariz Geriatr Soc J. 2003;8(3):3-12.
- Yozwiak ML, Lundergan LL, Kerrick SS, Galgiani JN. Symptoms and routine laboratory abnormalities associated with coccidioidomycosis. West J Med. 1988;149(4):419-21. [PubMed]
- Wieden MA, Lundergan LL, Blum J, et al. Detection of coccidioidal antibodies by 33-kDa spherule antigen, Coccidioides EIA, and standard serologic tests in sera from patients evaluated for coccidioidomycosis. J Infect Dis. 1996;173(5):1273-7. [CrossRef] [PubMed]
- Kuberski T, Herrig J, Pappagianis D. False-positive IgM serology in coccidioidomycosis. J Clin Microbiol. 2010;48(6):2047-9. [CrossRef] [PubMed]
- Blair JE, Currier JT. Significance of isolated positive IgM serologic results by enzyme immunoassay for coccidioidomycosis. Mycopathologia. 2008;166(2):77-82. [CrossRef] [PubMed]
- Santelli AC, Blair JE, Roust LR. Coccidioidomycosis in patients with diabetes mellitus. Am J Med. 2006;119(11):964-9. [CrossRef] [PubMed]
- Blair JE, Mayer AP, Currier J, Files JA, Wu Q. Coccidioidomycosis in elderly persons. Clin Infect Dis. 2008;47(12):1513-8. [CrossRef] [PubMed]
- Ampel NM, Giblin A, Mourani JP, Galgiani JN. Factors and outcomes associated with the decision to treat primary pulmonary coccidioidomycosis. Clin Infect Dis. 2009;48(2):172-8. [CrossRef] [PubMed]
- Blair JE, Chang YH, Cheng MR, et al. Characteristics of patients with mild to moderate primary pulmonary coccidioidomycosis. Emerg Infect Dis. 2014;20(6):983-990. [CrossRef] [PubMed]
- Galgiani JN, Ampel NM, Blair JE, et al.; Infectious Diseases Society of America. Coccidioidomycosis. Clin Infect Dis. 2005;41(9):1217-23. [CrossRef] [PubMed]
- Kerrick SS, Lundergan LL, Galgiani JN. Coccidioidomycosis at a university health service. Am Rev Respir Dis. 1985;131(1):100-2. [PubMed]
Additional Selected References
- Ampel NM. Coccidioidomycosis in persons infected with HIV-1. Ann N Y Acad Sci. 2007;1111:336-42. [CrossRef] [PubMed]
- Bergstrom L, Yocum DE, Ampel NM, et al. Increased risk of coccidioidomycosis in patients treated with tumor necrosis factor alpha antagonists. Arthritis Rheum. 2004;50:1959-66. [CrossRef] [PubMed]
- Blair JE, Kusne S, Carey EJ, Heilman RL. The prevention of recrudescent coccidioidomycosis after solid organ transplantation. Transplantation. 2007;83:1182-1187. [CrossRef] [PubMed]
- Blair JE, Mulligan DC. Coccidioidomycosis in healthy persons evaluated for liver or kidney donation. Transpl Infect Dis. 2007;9:78-82. [CrossRef] [PubMed]
- Braddy CM, Heilman RL, Blair JE. Coccidioidomycosis after renal transplantation in an endemic area. Am J Transplant. 2006;6:340-5. [CrossRef] [PubMed]
- Comrie AC. Climate factors influencing coccidioidomycosis seasonality and outbreaks. Environ Health Perspect. 2005;113:688-92. [CrossRef] [PubMed]
- Deresinski S. Coccidioides immitis as a potential bioweapon. Semin Respir Infect. 2003;18:216-9. [PubMed]
- Flaherman VJ, Hector R, Rutherford GW. Estimating severe coccidioidomycosis in California. Emerg Infect Dis. 2007;13:1087-90. [CrossRef] [PubMed]
- Hirschmann JV. The early history of coccidioidomycosis: 1892-1945. Clin Infect Dis. 2007;44:1202-7. [CrossRef] [PubMed]
- Johnson RH, Einstein HE. Amphotericin B and coccidioidomycosis. Ann N Y Acad Sci. 2007;1111:434-41. [CrossRef] [PubMed]
- Johnson RH, Einstein HE. Coccidioidal meningitis. Clin Infect Dis. 2006;42:103-7. [CrossRef] [PubMed]
- Laniado-Laborin R. Coccidioidomycosis and other endemic mycoses in Mexico. Rev Iberoam Micol. 2007;24:249-58. [PubMed]
- Pappagianis D. Coccidioidomycosis in California state correctional institutions. Ann N Y Acad Sci. 2007;1111:103-11. [CrossRef] [PubMed]
- Saubolle MA. Laboratory aspects in the diagnosis of coccidioidomycosis. Ann N Y Acad Sci. 2007;1111:301-14. [CrossRef] [PubMed]
- Stevens DA, Clemons KV. Azole therapy of clinical and experimental coccidioidomycosis. Ann N Y Acad Sci. 2007;1111:442-54. [CrossRef] [PubMed]
- Sunenshine RH, Anderson S, Erhart L, et al. Public health surveillance for coccidioidomycosis in Arizona. Ann N Y Acad Sci. 2007;1111:96-102. [CrossRef] [PubMed]
Reference as: Galgiani JN. Valley fever (coccidioidomycosis): turtorial for primary care physicians. Southwest J Pulm Crit Care. 2015;10(5):265-88. doi: http://dx.doi.org/10.13175/swjpcc073-15 PDF PDF in booklet form