
May 2025 Critical Care Case of the Month: Where’s the Rub?
Ethan Weisman
The University of Arizona College of Medicine – Phoenix
Phoenix, AZ USA
Chief Complaint: A 70-year-old woman with a 13-year history of Crohn’s disease presented with two days of severe generalized myalgias, progressive pleuritic chest pain and malaise, followed by the acute onset of confusion and oxygen desaturation.
History of Present Illness: She had been admitted one week earlier with bloody diarrhea and cramping lower abdominal pain, presumptively diagnosed with a Crohn’s flair and treated with solumedrol 40mg Q12 hourly. An esophagogastroduodenoscopy (EGD) and colonoscopy were performed on the second hospital day, showing angiodysplastic gastric lesions with stigmata of recent bleeding, and severe inflammation with serpentine ulceration of the rectum through the cecum. The angiodysplastic lesions were treated with argon plasma coagulation and colonic biopsies were performed. The patient received 2 units of packed red blood cells. She was discharged the next day on prednisone 40mg and pantoprazole 40mg daily.
She was only home a few hours when she experienced onset of severe generalized myalgias, pleuritic chest pain and malaise, with no change in her resolving gastrointestinal symptoms. She denied fever, cough or dysuria. A home test for SARS-CoV-2 was positive.
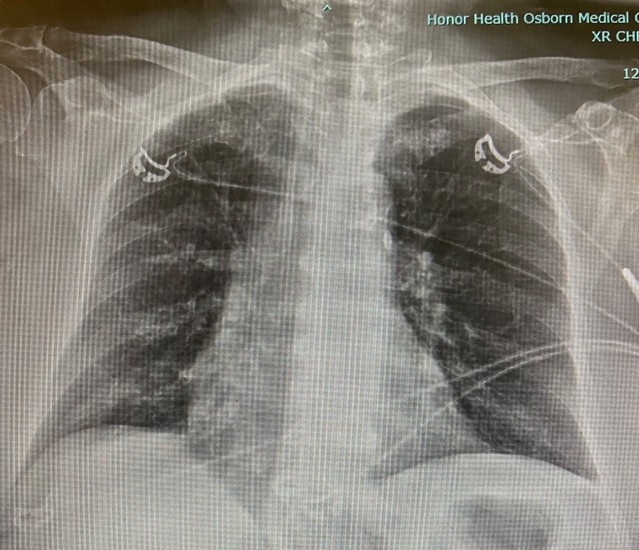
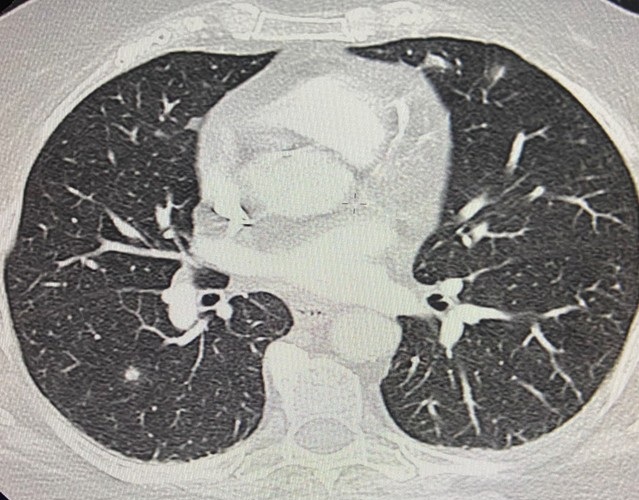
The next day she reported to the emergency room (ER) with worsening symptoms described above. She was afebrile with normal vitals and SpO2 of 93% on room air. The physical examination recorded only mild abdominal tenderness. Her white blood cell count (WBCC) was 15.9 109/L and Hb 12.7 g/dL. A chest x-ray (CXR) was clear and a CT angiogram of the chest showed no pulmonary embolism, but a few scattered nodules <1cm in diameter were noted throughout her lungs (Figures 1 and 2).
 Figure 1. CXR from ER visit. To view Figure 1 in a separate, enlarged window click here.
Figure 1. CXR from ER visit. To view Figure 1 in a separate, enlarged window click here.
 Figure 2. Representative image from thoracic CT scan done during ER visit. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Representative image from thoracic CT scan done during ER visit. To view Figure 2 in a separate, enlarged window click here.
The patient checked herself out of the ER against medical advice.
Two days later, the patient was returned to the hospital by her family, who reported she had become confused and had an SpO2 of 78% according to an oximeter they had purchased at a drug store.
Past Medical History: Her past medical history was significant for type-2 diabetes, hypertension and osteoporosis s/p bilateral hip arthroplasties. She was taking alendronate, empagliflozin, levothyroxine, losartan, metformin and a prednisone taper.
Physical Examination: Her temperature was 97.9o F., blood pressure 103/65 mmHg, heart rate 107 bpm, respiratory rate 26 bpm, and SpO2 92% on room air. She was described as ill-appearing and alert but disoriented. Her lungs were clear. Cardiac exam was normal except for tachycardia. Mild abdominal distention and tenderness were noted. The rest of the recorded examination was unremarkable.
What should be done next? (Click on the correct answer to be directed to the second of six pages)
 Post a Comment
Post a Comment

{kind=link}
{kind=link}
{kind=link}
{kind=link}