
RIGHT PLEURAL INSERTION OF A SMALL BORE FEEDING TUBE
Clement U. Singarajah
Tyler Glenn
Richard A. Robbins
Phoenix VA Medical Center, Phoenix, AZ
Reference as: Singarajah CU, Glenn T, Robbins RA. Right pleural insertion of a small bore feeding tube. Southwest J Pulm Crit Care 2011;2:71-6. (Click here for PDF version)
Abstract
We report a case of a 56 year old man who had a feeding tube inadvertently malpositioned into the right pleural space and had approximately 600 ml of tube feedings infused. After the malposition was recognized, the patient underwent chest tube placement, followed by video assisted thoracic surgery 5 days later. He made an uneventful recovery. The case illustrates the problems with identification and treating feeding tube insertion into the lung.
Case Presentation
History of Present Illness
A 56 year old male was transferred from another hospital where he had been admitted 9 days earlier for severe community acquired pneumonia secondary to penicillin sensitive Streptococcus pneumoniae, respiratory failure and sepsis syndrome. He had a past medical history of morbid obesity, type 2 diabetes mellitus, hepatitis C, hypertension and had received a pneumococcal vaccination 8 years earlier. His course was complicated by prolonged mechanical ventilation, hypotension resulting in oliguric acute renal failure and atrial fibrillation with a fast ventricular response requiring cardioversion. He had sufficiently improved with antibiotics, hemodialysis and supportive therapy that he was able to be transferred to our hospital. He had a prolonged but uncomplicated course in our intensive care unit (ICU). He was initially unable to be weaned from mechanical ventilation and underwent tracheostomy but was eventually able to tolerate tracheostomy collar and intermittent use of a tracheostomy tube with a speaking valve. He was noted to be intermittently confused and agitated. After 17 days in our ICU, transfer was planned to a general medical floor. However, prior to leaving our ICU he pulled his feeding tube and another small bore feeding tube was inserted. An abdominal film was performed and he was transferred to the medical floor. After transfer he complained through the night of chest pain and shortness of breath and required increasing inspired oxygen concentrations in order to maintain adequate oxygen saturation. .
Physical Examination
Physical examination was not markedly changed from the previous day. He had a tachycardia of 110, blood pressure of 139/97, respirations of 24, temperature of 36.3 degrees C and weight of 140.6 kilograms. He was not oriented to time or place and seemed to be in moderate discomfort. Pertinent findings including a small bore feeding tube in his left nostril, a tracheotomy in place and rhonchi over both lungs. Abdomen was protuberant but soft and there was no presacral or pretibial edema.
Laboratory Findings
Pertinent laboratory findings included arterial blood gases showing a pH of 7.44, pCO2 of 32 mm Hg, and pO2 of 65.3 on a FiO2 of 0.7. Blood glucose was elevated at 275 and his white blood cell count had increased from 6000/microL on the day of transfer to the floor to 11,400/microL with a left shift.
Radiography
Initial abdominal films are show in figure 1.
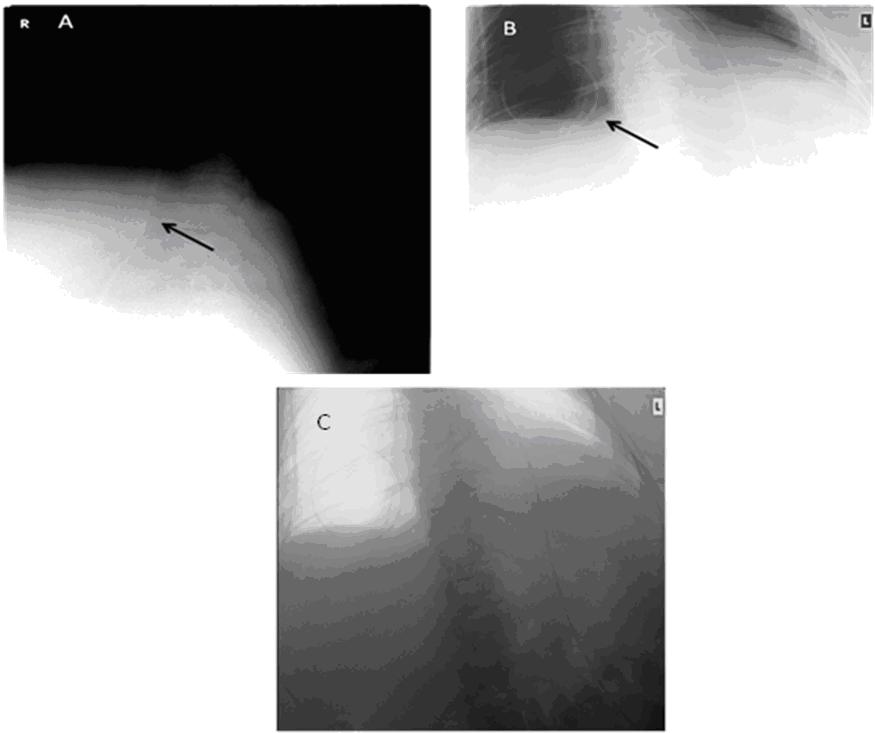
Figure 1. Panel A and B are abdominal x-rays taken for feeding tube placement. Panel A shows the feeding tube below the diaphragm indicated by the arrow. Panel B, labeled at the same time and with the same acquisition number does not show the tube below the diaphragm but shows a tube apparently in the right chest. Panel C is an inverted image of Panel B.
A chest X-ray was taken on the patient’s return to the intensive care unit (Figure 2).

Figure 2. A. Chest X-ray shows feeding tube in trachea and right mainstem bronchus, looping in lower right chest and extending to upper right chest (arrows). B. Inverted image of A.
Hospital Course
Because of his high oxygen requirements and dyspnea, the patient was placed on mechanical ventilation. Bronchoscopy confirmed that the tube was in the lung. Due to concern for a pneumothorax should the tube be removed, a chest tube was placed first and directed to drain the pleural effusion. The feeding tube was removed and a follow up chest x-ray confirmed a pneumothorax that was treated with another chest tube. It was estimated that about 600 ml of feeding formula had been infused into the chest. Approximately 700 ml of milky fluid consistent with feeding was collected by the thoracostomy tube. Thoracic surgery consultation was obtained and recommended video-assisted thoracic surgery which was performed 5 days latter. A small amount of what appeared to be feeding formula was removed. He made a slow and uneventful recovery and was discharged to an extended care facility after a total duration of 43 days in our hospital.
Discussion
Malposition of feeding tubes is relatively common (1,2). Given that the tubes are small, relatively flexible and blindly inserted this is not surprising. In a series of more than 2000 insertions, Sorokin and Gottlieb (1) reported a 2.4% rate of lung insertion while de Aguilar-Nascimento and Kudsk (2) found a 3.2% incidence of lung malposition. Most malpositions occurred in the intensive care unit with 95% of the patients having an abnormal mental status and more than half with an endotracheal tube. Therefore, our patient was typical of the patient prone for feeding tube malposition.
To prevent feeding tube malposition, many hospitals insert the tubes under fluoroscopic guidance (3). Perhaps more commonly, other hospitals require radiographic confirmation before beginning feeding (1,2) . The later is the policy at our hospital, but as this case illustrates, mishaps can occur even with this safeguard.
In our case, several errors were made leading to the adverse event. Although recorded at the same time, the initial abdominal films were actually taken at different times. The patient had pulled his first feeding tube and a second tube had been inserted by the ICU nurse into the lung. The medicine house officer who read the films was not informed that two films were taken and saw the tube below the diaphragm on the first film. The house officer missed the tube in the chest on the second film. However, on this and three subsequent films, all read by separate radiologists, the tube malposition was also not identified. It can be difficult with multiple densities, from chest cardiac leads, suction tubing, intravenous tubing, etc. to identify potentially misplaced feeding tubes.
Generally, feeding tube malposition is reasonably well tolerated although aspiration and pneumothorax may result (1-3). Removal of the tube usually results in little apparent clinical harm. Our case is unusual in that an enteral feeding formula was introduced into the pleural space. Although there are previous reports of pneumothorax complication feeding tube insertion, these are relatively uncommon and we were uncertain how to proceed (4). Eventually we decided on video assisted thoracic surgery with removal of any residual fluid. In this case the patient made an uneventful but prolonged recovery.
When a feeding tube is in the lung, it may or may not have punctured the pleura. If it has, as was clear in this case by the course it took, (multiple loops), the chance of a pneumothorax on removal may be high. It is a matter of opinion as to whether or not in this situation; a prophylactic chest tube should be placed prior to removal of the feeding tube. In this case, this was performed as he was on mechanical ventilation. In situations where the feeding tube is clearly in a mainstem bronchus, removal is probably safe without due concern for a pneumothorax.
The errors in the formal radiology readings may be reduced by inverting the images within the radiology viewing program, and making sure that the full course of the feeding tube from oropharynx to tip is noted. In some obese patients, such as this one, an abdominal x-ray and chest x-ray may be required to do this.
References
1. Sorokin R, Gottlieb JE. Enhancing patient safety during feeding-tube insertion: a review of more than 2,000 insertions. JPEN J Parenter Enteral Nutr 2006;30:440-5.
2. de Aguilar-Nascimento JE, Kudsk KA. Clinical costs of feeding tube placement. JPEN J Parenter Enteral Nutr 2007;31:269-73.
3. Huerta G, Puri VK. Nasoenteric feeding tubes in critically ill patients (fluoroscopy versus blind). Nutrition 2000;16:264-7.
4. Wendell GD, Lenchner GS, Promisloff RA. Pneumothorax complicating small-bore feeding tube placement . Arch Intern Med 1991;151:599-602.
 Post a Comment
Post a Comment
Reader Comments