
Doggonit! A Classic Case of Severe Capnocytophaga canimorsus Sepsis
Brittany Denzer MD1
Minh Do MD1
Alexandra N. Fuher MD1
Logan Harper MD2
Kaleigh Lindholm MD3
Kara Calhoun MD MPH4
Kara Mould MD MPH4,5
1Department of Internal Medicine, University of Colorado Anschutz Medical Campus (Aurora) (Denzer, Do, Fuher)
2Department of Family Medicine, University of Colorado Anschutz Medical Campus (Aurora) (Harper)
3Department of Pathology, Denver Health (Denver) (Lindholm)
4Department of Pulmonary Sciences and Critical Care Medicine, University of Colorado Anschutz Medical Campus (Aurora) (Calhoun, Mould)
5Department of Medicine, Division of Pulmonary, Critical Care & Sleep Medicine, National Jewish Health (Denver) (Mould)
Abstract
Capnocytophaga canimorsus is a commensal organism often found in the oropharyngeal tracts of dogs and cats, capable of causing significant morbidity and mortality in immunocompromised patients. Early identification of C. canimorsus is challenging due to the organism’s rare presentation, rapid clinical progression, and slow growth on microbiological media. We present a case of a 47-year-old man with exposure to snakes and dogs, and history of severe alcohol use disorder, who presented to the emergency department with acute generalized abdominal pain. His course was notable for progressive respiratory failure requiring intubation and multi-pressor septic shock with minimal response to initial broad-spectrum antibiotics, complicated by hypoglycemia and DIC with purpura fulminans. Multidisciplinary review of the peripheral smear, notable for long, thin, intra and extracellular gram-negative rods, rapidly characterized our pathogen as an atypical gram-negative rod. With additional review of medical history and zoonotic exposures, we were able to quickly identify and address our concern for C. canimorsus, broadening our antibiotics to account for resistance patterns particular to this organism.
Case Presentation
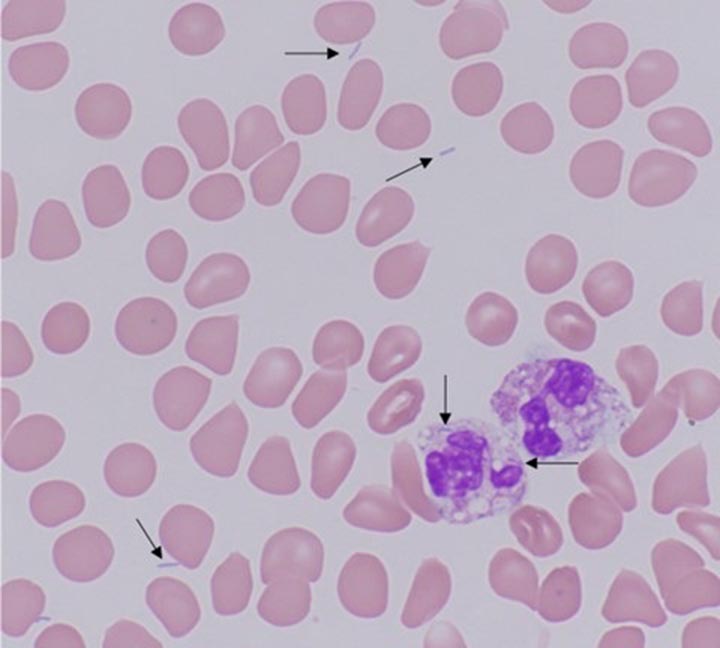
A 47-year-old man with severe alcohol use disorder and exposure to pet dogs and snakes presented to the emergency department with one day of generalized abdominal pain. He was normotensive, febrile (39.5°C), tachycardic (151 beats/minute), and in respiratory distress with tachypnea (44 breaths/minute) and hypoxia (70% SpO2 on room air). His exam was notable for bibasilar rales and a diffusely tender abdomen with rigidity and guarding. There was an inch-long superficial laceration on the patient’s left anterior thigh. Labs were notable for WBC 4.1k/uL, hemoglobin 14.9g/dL, platelets 33k/uL, glucose 36mg/dL, lactate 10.8mmol/L, AST 115U/L, ALT 48U/L, alkaline phosphatase 111U/L, PT 27.4 seconds, PTT 136 seconds, D-dimer >20ug/mL, and fibrinogen 151mg/dL. Chest radiograph demonstrated bibasilar airspace opacities. CT abdomen and pelvis showed gallbladder wall thickening and edema without gallstones. A peripheral blood smear showed long, thin, intra and extracellular gram-negative rods (Figure 1).

Figure 1. Peripheral blood smear with findings of long, thin, intra- and extracellular gram-negative rods, identified with arrows. To view Figure 1 in a separate, enlarged window click here.
Hospital Course
Metronidazole and levofloxacin were started in the emergency department for gram-negative sepsis with concern for gastrointestinal source. A dextrose infusion was started for hypoglycemia and hematology was consulted for disseminated intravascular coagulation (DIC). The patient developed rapid respiratory failure requiring intubation, so antibiotics were broadened with the addition of vancomycin and cefepime, and the patient was admitted to the medical intensive care unit. Subsequently, blood culture multiplex PCR returned negative for common organisms, including Salmonella, initially of concern due to his recent snake exposure. On day two, he developed multipressor shock and a purpuric rash involving his extremities (Figure 2).

Figure 2. Purpuric skin findings involving bilateral upper and lower extremities. To view Figure 2 in a separate, enlarged window click here.
Further history revealed the scratch on his thigh was from a dog. A multidisciplinary review of the case involving pathology, infectious disease, and intensive care teams identified Capnocytophaga canimorsus as an organism of concern given its consistence with the peripheral smear organism, as well as the clinical presentation of shock, DIC, and purpura fulminans in a patient with a dog scratch and alcohol use disorder. Antibiotics were changed to imipenem and levofloxacin with rapid improvement over the next several hours, weaning of vasopressors, and extubation. Antibiotics were further narrowed to ertapenem, then ampicillin-sulbactam after a penicillin allergy was deemed low risk. After twelve days of growth, blood cultures grew anaerobic gram-negative bacilli consistent with Capnocytophaga canimorsus.
Discussion
C. canimorsus is a bacteria found in the oropharyngeal tracts of dogs and cats; transmission is often associated with bites, scratches, or close contact with infected hosts, though there are also cases without documented animal contact (1). C. canimorsus causes significant disease in immunosuppressed patients and with asplenia or chronic heavy alcohol use (1,2). C. canimorsus infections carry a high mortality rate, estimated as high as fifty-five percent in septic patients (3,4). Unfortunately, identification of C. canimorsus is challenging and frequently delayed due to the organism's rare presentation and slow growth on microbiological media.
This case highlights a classic presentation of severe C. canimorsus infection including shock, hypoglycemia, DIC with purpura fulminans in a patient with heavy alcohol use and a recent dog scratch. In addition to early recognition of these typical features, multidisciplinary review of peripheral smear was essential to early suspicion for C. canimorsus.
DIC is seen in approximately 13% of C. canimorsus cases and is associated with high mortality (2,5). Purpura fulminans is a rare manifestation of DIC characterized by microvascular thrombosis leading to skin necrosis (5). Complications of purpura fulminans include gangrene, often requiring amputation, which was later seen with our patient, and contributes to significant disability.
C. canimorsus is often treated initially with broad spectrum antibiotics given its fastidious growth (3). Our patient declined despite escalating spectrum of antibiotics including levofloxacin, metronidazole, vancomycin, and cefepime, but rapidly improved following change to imipenem and levofloxacin, which was further narrowed to ertapenem, then ampicillin-sulbactam. This may be explained by resistant beta-lactamase producing strains of Capnocytophaga species, which are increasingly reported (3). Due to resistance, a carbapenem or beta-latamase inhibitor combination antibiotic is recommended (3). Early consideration of resistance patterns of C. canimorsus is essential in decreasing risk of complications associated with this organism (3,5).
Multidisciplinary review of the peripheral smear showing long, thin, intra- and extracellular gram-negative rods was essential for our early suspicion for C. canimorsus. With specific growth conditions and mean culture positivity of six days, traditional culture techniques making timely identification of C. canimorsus challenging. (2,4). In the case above, final identification by culture did not occur until the twelfth day of admission; notably, PCR testing is not standardly available and MALDI-TOF failed to provide earlier identification. Therefore, interdisciplinary review of the peripheral smear and recognition of classic clinical features of C. canimorsus infection proved critical in our rapid identification of the culprit organism.
Teaching Points:
- Capnocytophaga canimorsus is a bacterium commonly found in dog mouths, capable of causing devastating disease in immunocompromised patients.
- Severe presentations may include septic shock, hypoglycemia and DIC, and are associated with significant morbidity and mortality.
- Early identification of C. canimorsus is often challenging due to the organism's rare presentation and slow growth on microbiological media. Peripheral smear may be of diagnostic value in bacteremic patients.
- It is critical that providers maintain a high clinical suspicion for C. canimorsus in at-risk patients and treat them with antibiotics that consider possible resistance patterns.
References
- Chesdachai S, Tai DBG, Yetmar ZA, Misra A, Ough N, Abu Saleh O. The Characteristics of Capnocytophaga Infection: 10 Years of Experience. Open Forum Infect Dis. 2021 Apr 15;8(7):ofab175. [CrossRef][PubMed]
- Janda JM, Graves MH, Lindquist D, Probert WS. Diagnosing Capnocytophaga canimorsus infections. Emerg Infect Dis. 2006 Feb;12(2):340-2. [CrossRef][PubMed]
- Killington K, Lee N, Asher R, Farrant O, Stone N. Purpura fulminans secondary to Capnocytophaga canimorsus bacteraemia following a dog bite: A case report and review of literature. Access Microbiol. 2023 Jun 16;5(6):acmi000505.v3. [CrossRef][PubMed]
- Zajkowska J, Król M, Falkowski D, Syed N, Kamieńska A. Capnocytophaga canimorsus – an underestimated danger after dog or cat bite – review of literature. Przegl Epidemiol. 2016;70(2):289-295. [PubMed]
- Perera TB, Murphy-Lavoie HM. Purpura Fulminans. 2023 Jul 17. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. [PubMed]
 Post a Comment
Post a Comment
{kind=link}
{kind=link}
Reader Comments