Don’t Fire Sharon Helman-At Least Not Yet
Several developments have occurred over the past few days regarding prolonged wait times and secret lists at the Phoenix VA and its embattled director, Sharon Helman. President Obama has asked for an investigation and several Arizona Senators and Representatives have called for investigations and/or asked for the resignation of Helman and her administrative team (1,2). On 4/30/14, Dr. Robert Petzel, VA undersecretary for health, testified that an administrative team visited Phoenix soon after the controversy erupted and found “no evidence of a secret list… [or] patients who have died because they [were] on a wait list." (3). On 5/1/14 CNN posted an interview with Sharon Helman and her Chief of Staff, Dr. Darren Deering, who denied the allegations. Dr. Sam Foote, who made the original allegations, accused Helman and Deering of lying (4). CNN apparently confirmed Foote’s story with several sources inside the VA including a second physician, Dr. Katherine Mitchell (5). Later the same day, Eric Shinseki, Secretary of Veterans Affairs, suspended Helman and two others (5).
This all sounded very familiar (6). In 2012 the VA Office of Inspector General (OIG) issued a report on the accuracy of the Veterans Healthcare Administration (VHA) wait times for mental health services (7). The report found that “VHA does not have a reliable and accurate method of determining whether they are providing patients timely access to mental health care services. VHA did not provide first-time patients with timely mental health evaluations and existing patients often waited more than 14 days past their desired date of care for their treatment appointment. As a result, performance measures used to report patient’s access to mental health care do not depict the true picture of a patient’s waiting time to see a mental health provider.”
After the 2012 OIG report came the inevitable Congressional hearing (8). Although misrepresenting actual wait times has been known for many years, there has been inadequate action to correct the practice according to the VA OIG. Sen. Patty Murray, then chair of the Senate Committee on Veterans' Affairs, said the findings showed a "rampant gaming of the system." (8). A review of the OIG’s website revealed multiple instances of similar findings dating back to at least 2002 (6). In each instance, unreliable data regarding wait times was cited and no or inadequate action was taken.
The providers at the VA should not necessarily view this as not good news. The VA has usually sought to refocus blame away from the administrators to “lazy” or “poor” doctors. My guess is that we will soon see a number of accusations about Drs. Foote and Mitchell in an effort to administratively circle the wagons. VA administrators usually seize on such opportunities to control physicians. Remember the computer fiasco from several years back when an information technology administrator lost a computer with confidential patient information (9)? This not only resulted in information technology being placed in charge of the electronic healthcare record but a number of restrictions were placed on physician use of data. Furthermore, administrators can now not only regulate a physician’s salary but “black ball” physicians by false accusations through sources such as the National Practioner Data Bank (NPDB). Not surprisingly, physicians are reluctant to speak out when their livelihood can be threatened.
Clearly, the present system is not working. Firing Sharon Helman will solve nothing at the present other than giving some politicians the opportunity to congratulate themselves on weeding out a bad apple in this election year. Furthermore, firing Helman could be an attempt to hide a systemic problem by offering Helman as the “fall guy”. So instead of redoing the OIG investigations and the Congressional hearings which have accomplished nothing in the past, how about doing something else? Here are a few suggestions:
- Have Helman investigated by an independent source, not the OIG. Examine other VAs for similarly misrepresenting patient wait times. Over thirty years at the VA taught me that if wait times are being "gamed" by one VA, the times are also likely being "gamed" by others.
- Create a National Healthcare Administrator Data Bank similar to the NPDB with all the same safeguards and checks and balances available to physicians. Helman apparently had a history of misrepresenting data (10). It seems unlikely that she would have been hired if this was publically known.
- Provide adequate oversight. The local Veterans Integrated Service Network (VISN), VA Central Office in Washington, and Congress is not providing the oversight needed. Create a hospital board of directors consisting predominately of a majority of healthcare providers from the facility and Veterans (not to be appointed by the director) to provide oversight.
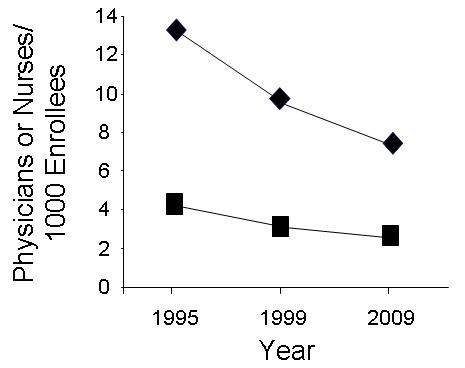
- Quit hiring more administrators while reducing the number of doctors. Inadequate numbers of providers is the root cause of prolonged wait times and has been present for a number of years (6). The numbers of administrators, nurses and doctors should be transparent and publically available.
- Quit paying administrators bonuses for work done by doctors. This only encourages cheating on reports (6,7). If administrators need a bonus, reward them for achievements in administrative efficiency or similar administrative goals. Both the criteria for and the amount of the bonus should be transparent and publically available.
- Scrap the VISN system. These local collections of administrators are another source of waste and appear to add no real oversight or patient benefit.
The optimist in me hopes the situation at the Phoenix VA and possibly other VAs is thoroughly investigated. If Helman is the “bad apple” many would like to portray-then fire her. If her actions are more a result of a systemic problem-then fix the problem. However, the cynic in me fears that Helman will be sacrificed without a thorough investigation and no change will occur. In that case I will again be writing about an investigation of VA administrators "gaming the system", probably in 2016.
Richard A. Robbins, MD*
Editor
Southwest Journal of Pulmonary and Critical Care
References
- Wagner D. McCain, Flake call for Senate probe of Phoenix VA. The Arizona Republic. April 23, 2014. Available at: http://www.azcentral.com/story/news/arizona/politics/2014/04/23/mccain-flake-call-senate-probe-phoenix-va/8061141/ (accessed 5/1/14).
- Harris C, Wagner D. Phoenix VA officials deny there's a secret wait list; doctor says they're lying. The Arizona Republic. April 29, 2014. Available at: http://www.azcentral.com/story/news/politics/2014/04/29/phoenix-va-director-congressman-call-for-removal/8447131/ (accessed 5/1/14).
- Wagner D. VA: We found no evidence to support allegations in Phoenix. The Arizona Republic. April 30, 2014. Available at: http://www.azcentral.com/story/news/politics/2014/04/30/phoenix-veteran-hospital-deaths-investigation/8518721/ (accessed 5/1/14).
- Bronstein S, Griffin D, Black N. Phoenix VA officials deny there's a secret wait list; doctor says they're lying. CNN. May 1, 2014. Available at: http://www.cnn.com/2014/04/30/health/veterans-dying-health-care-delays/ (accessed 5/1/14).
- Wagner D. Second VA doctor blows whistle on patient-care failures. The Arizona Republic. May 1, 2014. Available at: http://www.azcentral.com/story/news/investigations/2014/05/02/second-va-doctor-blows-whistle-patient-care-failures/8595863/ (accessed 5/1/14).
- Robbins RA. VA administrators gaming the system. Southwest J Pulm Crit Care 2012;4:149-54.
- VA Office of Inspector General. Review of Veterans’ Access to Mental Health Care. 1.http://www.va.gov/oig/pubs/VAOIG-12-00900-168.pdf (accessed 5-1-14).
- Vogel S. VA mental health system sharply denounced at hearing. Washington Post. April 25, 2012. Available at: http://www.washingtonpost.com/politics/va-mental-health-system-sharply-denounced-at-hearing/2012/04/25/gIQAXG3mhT_story.html (accessed 5/1/14).
- Lee C, Goldfarb ZA. Stolen VA laptop and hard drive recovered. Washington Post. June 30, 2006. Available at: http://www.washingtonpost.com/wp-dyn/content/article/2006/06/29/AR2006062900352.html (accessed 5/1/14).
- Corbin C. Arizona VA boss accused of covering up veterans' deaths linked to previous scandal. Foxnews.com. April 24, 2014. Available at: http://www.foxnews.com/politics/2014/04/24/arizona-va-boss-accused-covering-up-veterans-deaths-linked-to-previous-scandal/ (accessed 5/1/14).
*The views expressed are those of the author and do not necessarily reflect the views of the Arizona, New Mexico, Colorado, or California Thoracic Societies or the Mayo Clinic.
Reference as: Robbins RA. Don't fire Sharon Helman-at least not yet. Southwest J Pulm Crit Care. 2014;8(5):275-7. doi: http://dx.doi.org/10.13175/swjpcc060-14 PDF
 Rick Robbins, M.D.
Rick Robbins, M.D.