
National Health Expenditures: The Past, Present, Future and Solutions
Richard A. Robbins, MD
Phoenix Pulmonary and Critical Care Research and Education Foundation
Gilbert, AZ
"[T]he US health care system … defies the laws of economics, and of gravity. Once the price is high, it just stays there."- Dr. Naoki Ikegami
Abstract
The costs of health care in the US have been increasing for many years and the US now spends more on health care than other developed country. The cost of health care is higher in the US in nearly every category. However, the dramatic rise in health care costs over the past 35 years occurs during the time when pharmaceutical costs and administrative costs have also dramatically risen. It seems likely that these costs may account for much of the increase in health care. However, neither is dealt with by the Affordable Care Act (ACA). Until a system of oversight is enacted on medical costs, it seems likely that US health care costs will continue to rise.
The Past
In comparison to other economically developed countries health care costs have risen dramatically in the US over the past 35 years (Figure 1) (1).
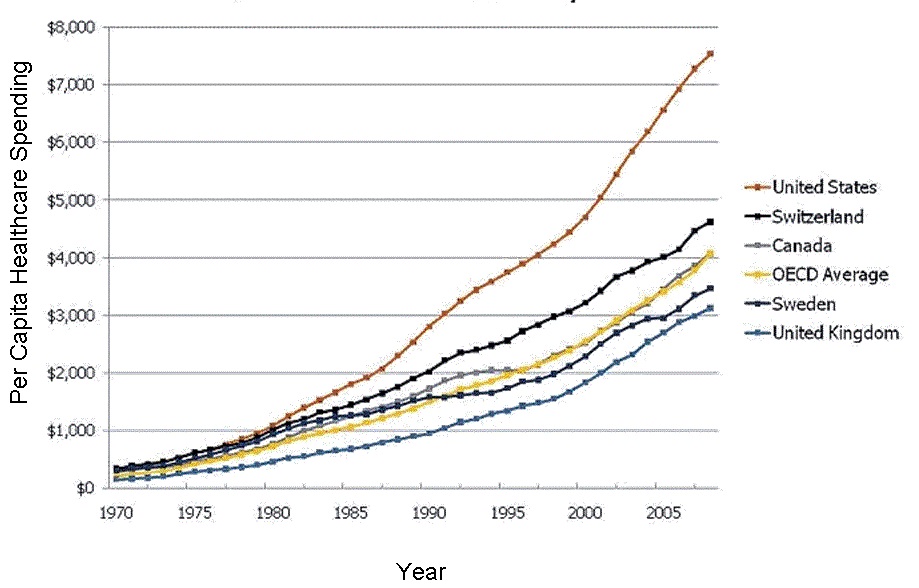
Figure 1. Rise in health care spending in the US and selected other countries.
Myths. The reasons for this rise in spending have been shrouded in myths and accusations. It has been argued that high costs is the price for the best health-care system in the world. However, patient outcomes in the US are mixed. In a 2011 report by the Organization for Economic Co-operation and Development (OECD), the United States ranked 25th in life expectancy (1). Although we do better in cancer survival rates, we are more likely to die of heart disease and we do not have a good track record on treating chronic diseases such as asthma.
Health care rationing. An argument has been made that because health care is heavily rationed in other countries, Americans use more health-care services in comparison. We do rank high in the use of some expensive tests and procedures (more on this later), but overall the OECD reports that the US is well below other developed countries in number of average doctor visits per year, hospitalizations and hospital length of stay (1). Americans have better-than-average access to specialists, but we lag compared to other countries in getting immediate access to a primary care doctor when we're sick and we are much more likely forgo heath care because of costs (2).
Bad patients. Some have claimed that the US has to spend more on health care because we are fat and lazy. Although this may be true, it does not explain the gap in health care spending between the US and other countries. Obesity rates are higher in the US but the US compares well to other countries in smoking and drinking (1). We also have a younger population compared to many other OECD countries which should actually lower costs (1).
Tort reform. The US has more lawyers and more lawsuits of doctors but this does not seem to be a major factor in health care costs. Tort reform would probably not go far in bringing down US health-care costs. A 2009 study by the nonpartisan Congressional Budget Office (CBO) found that implementing tort reform would reduce US health care spending by only 2 percent (3).
Government inefficiency. There is also speculation that US Government inefficiency and spending that drives up health care costs. Health care administrative costs in the Veterans Administration (VA) are estimated to be lower than private insurance according to the CBO (4). However, as recently discovered in the patient wait times scandal, VA data may be suspect. The Centers for Medicare and Medicaid Service's (CMS) administrative costs are reported to be about 2 percent of claims costs, while private insurance companies’ administrative costs are in the 20 to 25 percent range. The argument is that private industry with costs for advertising, collection, and profit are eliminated by CMS resulting in lower costs. However, this concept has also been challenged. CMS’s administrative costs are often hidden or completely ignored by the complex and bureaucratic reporting and tracking systems used by CMS (5). Furthermore, the estimates completely ignore the inefficiencies created by CMS's mandates requiring an increasingly heavy paperwork burden for physicians and hospitals.
Physician income. Some think that greedy physicians making too much money explain the rising costs in health care. Physician compensation varies widely between specialty, health care setting and region. Laugesen and Glied (6) concluded that higher physician fees were the main drivers of higher US spending. However, in 1970, the average inflation-adjusted income of general practitioners was $185,000. In 2010, it was $161,000, despite a near doubling of the number of patients that doctors see a day. Furthermore, during the boom years of the 1990's physician incomes remained relatively stagnant with an actual decline in the early 2000's (7-9). Although physician income is higher in the US than other countries, it would not appear to explain increasing health care costs since physician income was predominately stagnant or decreasing while health care costs rose.
Drug costs. Pharmaceutical costs have been increasing in the US (Figure 2) (10).
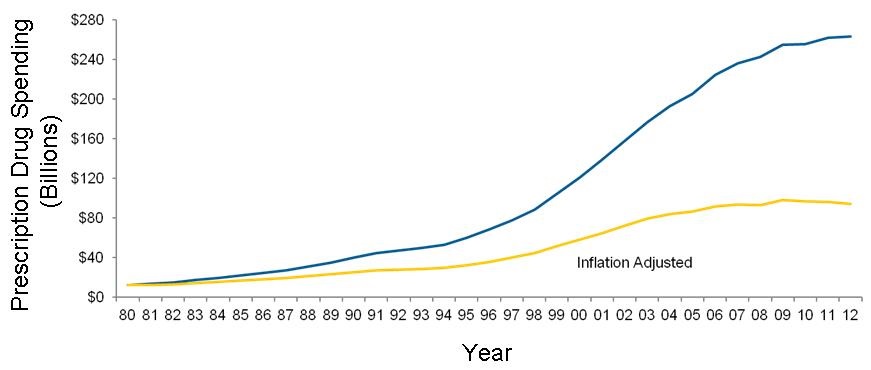
Figure 2. Total prescription drug spending 1980-2012.
Some have blamed these costs in increasing health care costs in the US. Although the rate of growth appears to be leveling off when adjusted for inflation (Figure 2), pharmaceutical costs remain high in the US.
Administrative costs. In ground-breaking work published in 1991 Woolhandler and Himmelstein (11) found that US administrative health care costs increased 37% between 1983 and 1987. They estimated these costs accounted for nearly a quarter of all health care expenditures. In Canada the administrative costs were about half as much and declined over the same period. They followed their 83-87 report by examining data from 1999 (12). US administrative costs had risen to 31% of US health care expenditures.
The trend is perhaps best illustrated by the graph below (Figure 3) (13).
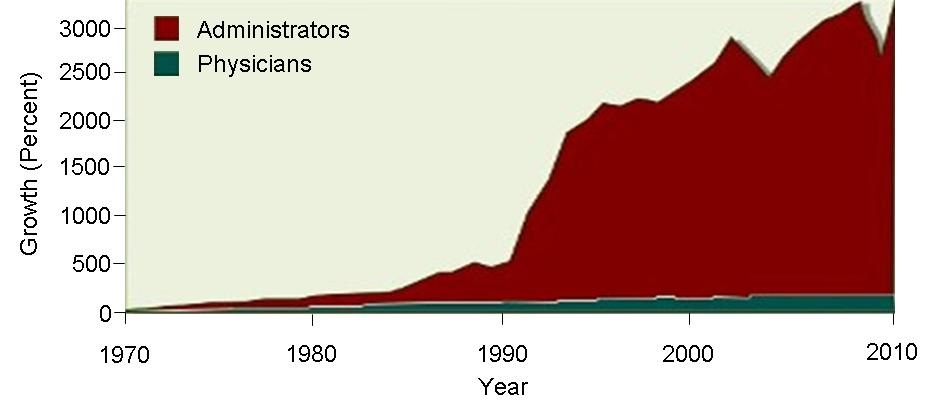
Figure 3. Growth in administrators and physicians 1970-2010 (used with permission of David Himmelstein).
The growth in administrative costs may not limited to the private sector. CMS' administrative costs are very difficult to determine. Similarly, the VA also has hidden costs. However, during my 30 years at the VA, I saw a disturbing growth in the front office. New assistant directors were continually hired, sometimes during a hiring freeze when needed doctors and nurses were not hired (Robbins RA, unpublished observations). The growth in VA administration has been staggering at some levels. Regional Veterans Integrated Service Network (VISN) offices were founded in the mid 1990's. However, these VISNs provide no healthcare and now number nearly 5000 employees (14). VA central office in Washington grew from about 800 employees to 11,000 in the last 15 years (14). This represents a staggering 20-fold increase over the past 15 years.
The Present
High Costs. Nearly everyone agrees that health care costs are too high and have continued to rise albeit more slowly during the Obama administration (1,15). At $8713 per person the US outspent every other OECD country for a number of years including 2015 (Figure 4) (1,15).
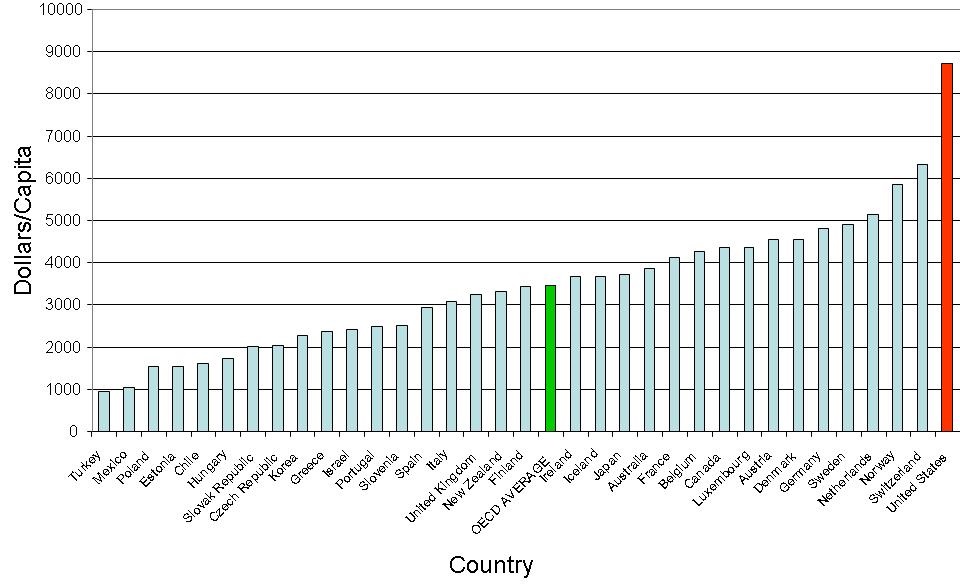
Figure 4. Current expenditure on health, per capita, US$ purchasing power parities. OECD average in green and United States in red.
The next closest was Switzerland at $6325. The US is a very rich country, but even so, it has devoted an increasing percentage of its gross domestic product (GDP) to health than any other country for a number of years including 2015 (Figure 5).
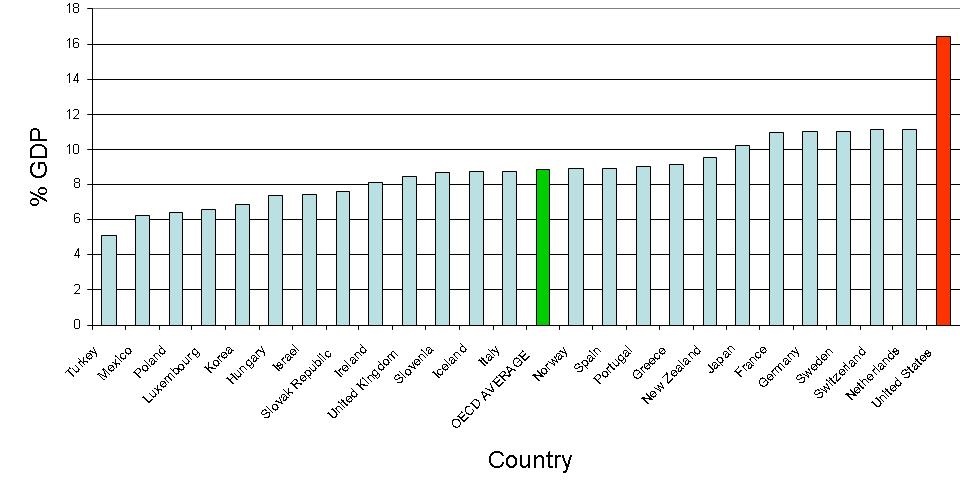
Figure 5. Current expenditure on health as a % of gross domestic product (GDP). OECD average in green and United States in red.
Switzerland is the next highest, at 11.1% of GDP, and the average among economically developed countries was almost half that of the US, at 8.9%.
High Numbers of Expensive Procedures. There is plenty of blame to spread for the increased cost of health care in the US. Spending on almost every area of health care is higher (Figure 6) (1,2).
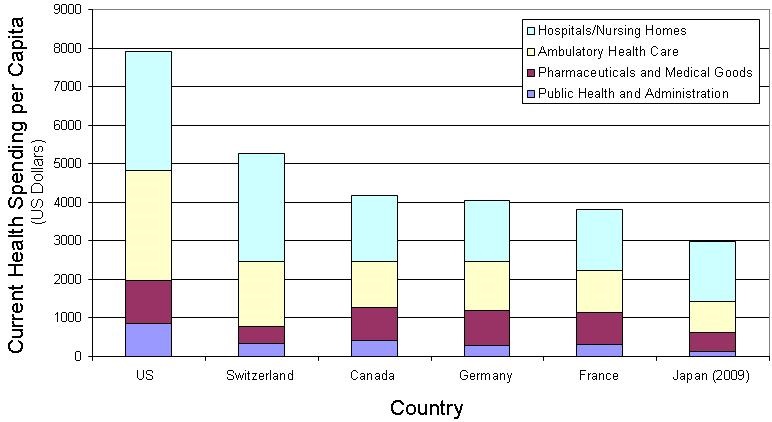
Figure 6. Health spending by category in US dollars 2010 or latest year available.
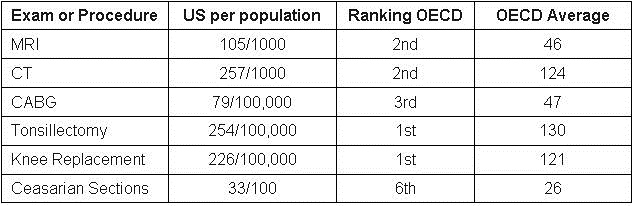
Because the spending is higher in nearly every category, the reasons for the high costs in the US are likely multifactorial. US health care has a long-standing reputation for excessive numbers of procedures at high costs. The data would seem to back that impression. The numbers of some expensive procedures or operations appear to be higher in the US compared to other countries (Table 1) (1).
Table 1. Numbers of exams or procedures in the US with OECD rank and average.
High Cost per Procedure. Furthermore, the costs of procedures in the US are high compared to other countries (1,16). (Table 2).
Table 2. Cost of common procedures. Highest cost in red.
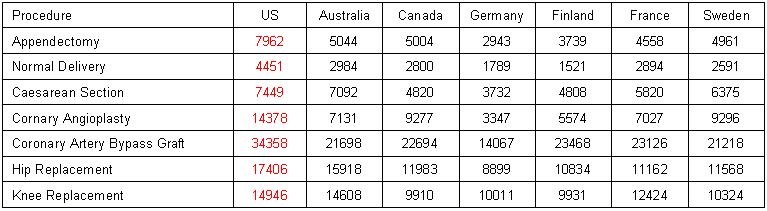
The average price for a wide range of both medical and surgical services in the US is 85 percent higher than other OECD countries (16). Both the numbers of expensive procedures and the high cost of procedures undoubtedly contribute to the high cost of health care in the US.
Administrative Costs. In 1999 the administrative costs of health care were estimated to be about 1/3 of all costs and were rapidly rising. There appears to have been little slow down in the rapid rise of administrative costs. Himmelstein and Woolhandler (17) estimated that administration costs could be as much as 45% of health care costs in 2014. There is no line for administrative costs on a medical bill but these costs are factored into all categories of medical spending.
The Future
As both Niels Bohr and Yogi Berra have said, "it's tough to make predictions, especially about the future". Now that King vs. Burwell has been settled, it is apparent that American health care will be directed by the ACA for the foreseeable future. Each year an official National Health Expenditure Projections for the next 10 years is released by the Centers for Medicare and Medicaid Services (CMS)’ Office of the Actuary. By examining these projections (which may be overly optimistic) as well as some observational studies, a rough prediction for the costs of health care can be made.
Economies of Scale. A principle in medical economics central to the Affordable Care Act (ACA) is economies of scale (18). The theory is that larger insurers will have lower prices because they are more administratively efficient. However, a recent study found that the largest insurer in each of the US states served by HealthCare.gov raised their prices in 2015 by an average of over 10% compared to smaller competitors in the same market (19). Those steeper price hikes for monthly premiums did not seem warranted by the level of health claims which did not significantly differ as a percentage of premiums in 2014.
Provider-Owned Health Plans. Another principle of the ACA in controlling health care costs is establishment of provider-owned (usually hospital) health plans. The theory is that substitution of provider-owned health plans will lower costs by controlling doctors over charging in a fee-for-service model. Although temptingly simple, a recent study concludes that this theory is not supported by the evidence. Comparing provider-owned to nonprovider-owned plans within twelve counties across the US was on average 12% more expensive compared to traditional insurers (20).
Drug Costs. Although drug prices remain consistently high in the US compared to other economically developed countries, competition to reduce these prices for CMS patients has been limited by Congress. Most health care plans have focused on formularies to control prices. Under this system, contracts with pharmaceutical manufacturers establish preferred drugs for use by their clients and their contracted physician prescribers. Although this strategy has been in place for some time, it appears to be ineffectual in controlling drug costs (Figure 6). Most countries place price controls on drugs, a strategy that seems to lack political will in the US (21). There appears to be little in the ACA that will control drug costs.
Administrative Costs. Himmelstein and Woolhandler (22) calculated new overhead costs from the official National Health Expenditure Projections for 2012-2022 released by the Centers for Medicare and Medicaid Services (CMS)’ Office of the Actuary in July 2014. Between 2014 and 2022, CMS projects $2.757 trillion in spending for private insurance overhead and administering government health programs (mostly Medicare and Medicaid), including $273.6 billion in new administrative costs attributable to the ACA. Nearly two-thirds of this new overhead—$172.2 billion—will go for increased private insurance overhead.
Most of this soaring private insurance overhead is attributable to rising enrollment in private plans which carry high costs for administration and profits. The rest reflects the costs of running the ACA exchanges.
Insuring the 25 million additional Americans, as the ACA is projected to do, is surely worthwhile, but the administrative cost is enormous. The ACA isn’t the first time we’ve seen bloated administrative costs from a federal program that subcontracts for coverage through private insurers. Medicare Advantage plans’ overhead averaged 13.7 percent in 2011, about $1,355 per enrollee. However, both Congress and the White House seem intent on sending more federal dollars to private insurers. Indeed, the House Republican’s initial budget proposal would have "voucherized" Medicare, eventually diverting almost the entire Medicare budget to private insurers. Fortunately, the measure passed by the House on April 30, 2015 dropped the voucher scheme.
Solutions
The difficulty with the ACA is that it does not appear to control the two major causes of the rise in health care spending - pharmaceutical costs and more importantly administrative costs. Himmelstein and Woolhandler (22) have long advocated a national single-payer system for health care similar to Canada's. They cite the low overhead for Medicare and Medicaid and the VA as demonstrating that such a system can work in the US. Despite the obfuscation of the overhead data by both US government agencies such as CMS and the VA, it seems likely that a single payer system would be more efficient than a private system. As Himmelstein and Woolhandler (22) have stated "public insurance gives much more bang for each buck".
However, a caveat must be added. A lesson that should be learned from the recent VA scandal is that public officials are no more honest that private companies in reporting data. Any system devised will need close oversight by knowledgeable patient care advocates. If not, the dollars intended for health care will be diverted into administrative pockets. It seems most likely that this should be on a local level by health care providers not employed or appointed by the administrators they oversee. Otherwise, there would be no real oversight. The ACA seems to encourage "provider-owned" health plans. These plans should be overseen not by the business cronies or administratively appointed physicians and nurses, but by independent health care providers who will look at administrative costs with a suspicious eye and question the costs at a local level. Otherwise the present system of less care at higher prices will persist.
References
- Organisation for Economic Co-operation and Development. Available at: http://www.oecd.org/ (accessed 8/4/15).
- Stokes B. Health affairs: among 11 nations, American seniors struggle more with health costs. Pew Research Center. December 3, 2014. Available at: http://www.pewresearch.org/fact-tank/2014/12/03/health-affairs-among-11-nations-american-seniors-struggle-more-with-health-costs/ (accessed 8/4/15).
- Congressional Budget Office. October 9, 2009. Available at: https://www.cbo.gov/sites/default/files/111th-congress-2009-2010/reports/10-09-tort_reform.pdf (accessed 8/4/15).
- Congressional Budget Office. Comparing the costs of the veterans’ health care system with private-sector costs. December, 2014. Available at: https://www.cbo.gov/sites/default/files/cbofiles/attachments/49763-VA_Health care_Costs.pdf (accessed 8/4/15).
- Mathews M. Medicare’s hidden administrative costs: a comparison of Medicare and the private sector. The Council for Affordable Health Insurance. January 10, 2006. Available at: http://www.cahi.org/cahi_contents/resources/pdf/CAHI_Medicare_Admin_Final_Publication.pdf (accessed 8/4/15).
- Laugesen MJ, Glied SA. Higher fees paid to US physicians drive higher spending for physician services compared to other countries. Health Aff (Millwood). 2011;30(9):1647-56. [CrossRef] [PubMed]
- Ballas C. Why do doctors accept gifts, and what would happen if they didn't? The Last Psychiatrist. October 26, 2010. Available at: http://thelastpsychiatrist.com/2010/10/why_do_doctors_accept_gifts.html (accessed 8/4/15).
- Tu HT, Ginsburg PB. Losing ground: physician income, 1995-2003. Track Rep. 2006;(15):1-8. [PubMed]
- Medscape physician compensation report 2015. Available at: http://www.medscape.com/features/slideshow/compensation/2015/public/overview#page=1 (accessed 8/4/15).
- Centers for Medicare & Medicaid Services, Office of the Actuary. Data released January 7, 2014. Available at: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/Downloads/Proj2012.pdf (accessed 8/4/15)
- Woolhandler S, Himmelstein DU. The deteriorating administrative efficiency of the US health care system. N Engl J Med. 1991;324(18):1253-8. [CrossRef] [PubMed]
- Woolhandler S, Campbell T, Himmelstein DU. Costs of health care administration in the United States and Canada. N Engl J Med. 2003;349(8):768-75. [CrossRef] [PubMed]
- Bureau of Labor Statistics. NCHS. Himmelstein and Woolhandler analysis of current population survey. Avaialable at: http://www.pnhp.org/ (accessed 8/4/15).
- Kizer KW, Jha AK. Restoring trust in VA health care. N Engl J Med 2014;371:295-7. [CrossRef] [PubMed]
- Kane J. Health costs: how the US compares with other countries. PBS Newshour. 2012. Available at: http://www.pbs.org/newshour/rundown/health-costs-how-the-us-compares-with-other-countries/ (accessed 8/4/15).
- Koechlin F, Lorenzoni L, Schreyer P. Comparing price levels of hospital services across countries: results of pilot study. OECD. Available at: http://www.oecd.org/officialdocuments/publicdisplaydocumentpdf/?cote=delsa/hea/wd/hwp(2010)4&doclanguage=en (accessed 8/4/15).
- Himmelstein D, Woolhandler S. The post-launch problem: the affordable care act’s persistently high administrative costs. May 27, 2015. Available at: http://healthaffairs.org/blog/2015/05/27/the-post-launch-problem-the-affordable-care-acts-persistently-high-administrative-costs/#table
- Robbins RA. Capture market share, raise prices. Southwest J Pulm Crit Care. 2015;11(2):88-9. [CrossRef]
- Wang E, Gee G. Larger Issuers, larger premium increases: health insurance issuer competition post-aca. Technology Science. 2015081104. August 11, 2015. Available at: http://techscience.org/a/2015081104 (accessed 8/31/15).
- Colemen K, Gleeson J. Cheapest healthcare provider-owned insurance plans still 12% more expensive than cheapest insurance plans not owned by providers. HealthPocket. August 20, 2015. Available at: https://www.healthpocket.com/healthcare-research/infostat/fee-for-service-and-provider-health-plans#.VeRqLPlVhBd (accessed 8/31/15).
- US Department of Commerce. Pharmaceutical price controls in OECD countries: implications for U.S. Consumers, pricing, research and development, and innovation. 2004. Available at: http://www.ita.doc.gov/td/chemicals/drugpricingstudy.pdf (accessed 8/31/2015).
- Himmelstein D, Woolhandler S. The post-launch problem: the affordable care act’s persistently high administrative costs. Health Affairs Blog. 5/27/2015. Available at: http://healthaffairs.org/blog/2015/05/27/the-post-launch-problem-the-affordable-care-acts-persistently-high-administrative-costs/ (accessed 8/31/15).
Cite as: Robbins RA. National health expenditures: the past, present, future and solutions. Southwest J Pulm Crit Care. 2015;11(4):176-85. doi: http://dx.doi.org/10.13175/swjpcc105-15 PDF
 Rick Robbins, M.D.
Rick Robbins, M.D.