
August 2024 Image of the Month: Lymphomatoid Granulomatosis
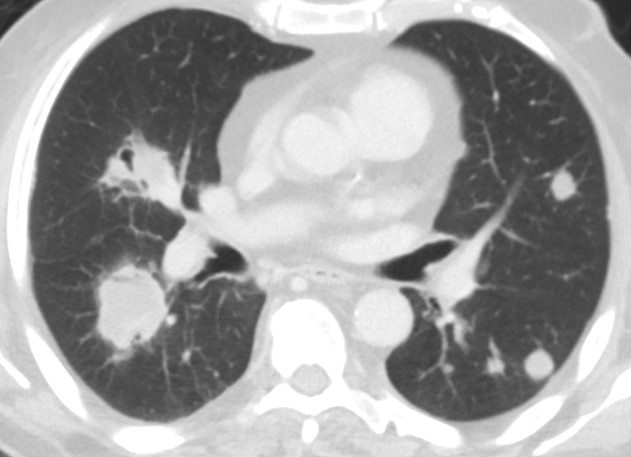
 Figure 1. Multiple bilateral pulmonary nodules and masses demonstrating a waxing and waning behavior when compared to an older outside CT scan. Some of the lesions demonstrate partial cavitation or contain air bronchograms. To view Figure 1 in a separate enlarged window click here.
Figure 1. Multiple bilateral pulmonary nodules and masses demonstrating a waxing and waning behavior when compared to an older outside CT scan. Some of the lesions demonstrate partial cavitation or contain air bronchograms. To view Figure 1 in a separate enlarged window click here.
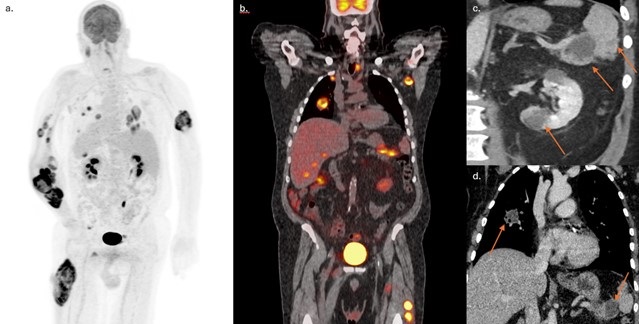
 Figure 2. FDG PET/CT MIP (A) and coronal fused (B) reconstructions highlighting extensive disease involvement including both visceral and soft tissue lesions. Coronal images from abdominal (C) and chest (D) contrast-enhanced CT scans demonstrate somewhat ill-defined hypoattenuating masses in the tail of the pancreas, spleen, left kidney, and a partially cavitary right superior lower lobe nodule. To view Figure 2 in a separate enlarged window click here.
Figure 2. FDG PET/CT MIP (A) and coronal fused (B) reconstructions highlighting extensive disease involvement including both visceral and soft tissue lesions. Coronal images from abdominal (C) and chest (D) contrast-enhanced CT scans demonstrate somewhat ill-defined hypoattenuating masses in the tail of the pancreas, spleen, left kidney, and a partially cavitary right superior lower lobe nodule. To view Figure 2 in a separate enlarged window click here.
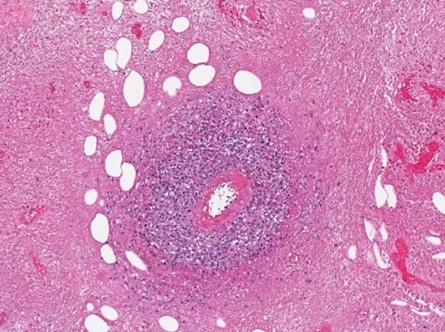
 Figure 3. Histopathologic evaluation demonstrated extensive coagulative necrosis with surrounding giant cells. Within the viable tissue, sheets of histiocytes and heterogeneous populations of lymphoid cells with prominent perivascular lymphohistiocytic infiltration were demonstrated. To view Figure 3 in a separate enlarged window click here.
Figure 3. Histopathologic evaluation demonstrated extensive coagulative necrosis with surrounding giant cells. Within the viable tissue, sheets of histiocytes and heterogeneous populations of lymphoid cells with prominent perivascular lymphohistiocytic infiltration were demonstrated. To view Figure 3 in a separate enlarged window click here.
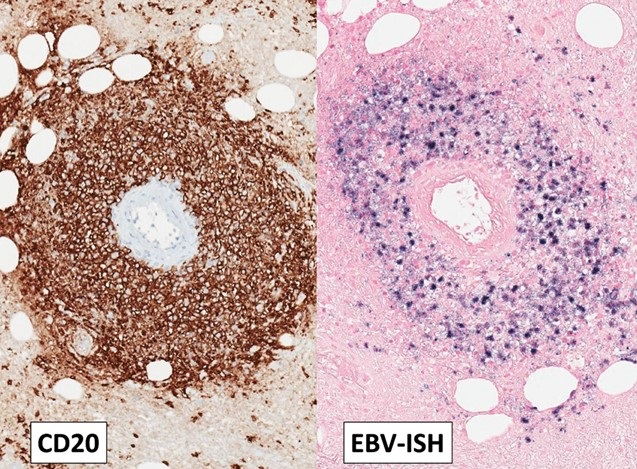
 Figure 4. Immunohistochemistry showed most lymphoid cells to be CD3 positive T-cells. Both individually scattered large B cells and a thick perivascular cuff of CD20 positive large B-cells were also noted throughout the lymphohistiocytic proliferation. Ebstein Barr Encoding Region (EBER) in situ hybridization showed that most of the large B-cells, both in the perivascular and diffuse distribution, were positive for Epstein-Barr virus (EBV) To view Figure 4 in a separate enlarged window click here.
Figure 4. Immunohistochemistry showed most lymphoid cells to be CD3 positive T-cells. Both individually scattered large B cells and a thick perivascular cuff of CD20 positive large B-cells were also noted throughout the lymphohistiocytic proliferation. Ebstein Barr Encoding Region (EBER) in situ hybridization showed that most of the large B-cells, both in the perivascular and diffuse distribution, were positive for Epstein-Barr virus (EBV) To view Figure 4 in a separate enlarged window click here.
A 72-year-old man with a history of hypertension and diabetes and a remote smoking history (10 pack-years) presented to our institution with approximately 1 year of poor appetite, night sweats, and progressive weakness as well as ~ 70 lb. weight loss over the past 6 months. He had also developed multiple intramuscular tumors within his extremities, with rapid growth of a right forearm tumor requiring fasciotomy and debridement. He denied recent foreign travel and his family history was significant for non-Hodgkin lymphoma in his father. Extensive prior clinical and laboratory investigation yielded a negative rheumatological workup, hypercalcemia and an elevated CRP, but was otherwise unremarkable.
Outside imaging studies had shown abdominal adenopathy with numerous intramuscular masses as well as several visceral masses involving the liver, pancreas, spleen and kidneys. Histopathology from several sources including his right forearm debridement surgical specimen and biopsy specimens from lesions in his lung, liver, and groin have all been nondiagnostic. Pathology reports from an outside institution describe the samples as demonstrating only granulomatous inflammation with necrotic debris. A chest CT was ordered to further characterize pulmonary nodules and masses seen on recent abdominal imaging. When compared to a prior outside CT scan, the lesions demonstrated some interval waxing and waning. Also, some of the lesions were cavitary and some contained air bronchograms (Figure 1). Given the waxing and waning behavior of the pulmonary nodules, the differential diagnosis included inflammatory pseudotumor, vasculitis, additional nonmalignant infiltrative processes, as well as hematologic malignancy. Many of the lesions scattered throughout the body were shown to be hypermetabolic on FDG PET-CT (Figure 2).
The patient came to our institution for multidisciplinary management. Surgical biopsy of a left thigh lesion was obtained. Histopathologic analysis showed extensive coagulative necrosis, however within the viable tissue there were sheets of histiocytes and heterogeneous populations of lymphoid cells. Immunohistochemistry staining showed most lymphoid cells to be CD3 positive T-cells with a thick perivascular cuff of CD20 positive large B-cells. Ebstein Barr Encoding Region (EBER) in situ hybridization showed the vast majority of the large B-cells to be positive for Epstein-Barr virus (EBV) (Figures 3 and 4). The histologic findings of extensive necrosis, granulomatous inflammation, and perivascular proliferation of EBV positive large B-cells was diagnostic of an EBV positive large B-cell lymphoma. In the clinical context of numerous mass like lesions involving multiple organs, including the lungs, soft tissue, kidney, spleen, and skeletal muscle, the findings were highly suggestive of lymphomatoid granulomatosis, grade 3. Diagnostic lumbar puncture for staging revealed no evidence of CNS involvement and the patient was subsequently initiated on an R-CHOP chemotherapy regimen given his substantial tumor burden.
Lymphomatoid granulomatosis (LYG) is an uncommon Ebstein-Barr virus (EBV) related entity that characteristically causes pulmonary nodules and lymphocytic angioinvasion. It falls on the spectrum of EBV-driven B-cell lymphoproliferative disease. LYG is defined and graded pathologically by the amount and density of EBV+ atypical B-cells while also having angioinvasive EBV- T-cell infiltrates (1). Classic organ involvement includes skin, lungs, central nervous system, liver, and kidneys with bone marrow and lymph nodes less likely. The disease most often affects middle-aged adults with men twice as likely to be affected compared to women. LYG classically involves immunocompromised hosts. Importantly, LYG and posttransplant lymphoproliferative disorder (PTLD) have nearly identical pathologic features; thus, transplant recipients should be diagnosed with PTLD (2).
One of the earliest studies on LYG found that malignant lymphoma developed in 12% of patients (3). A subsequent case series found that despite only four of their seven patients showing proof of monoclonality or oligoclonality, all cases of LYG behaved aggressively (4). Grading the EBV+ density guides treatment recommendations with low-grade being treated with interferon-α2b while high-grade is treated with immunochemotherapy. Hematopoietic stem cell transplant is considered for primary refractory disease or multiple relapses (1). Overall, treatment has remained controversial for decades. The mortality rate of LYG ranges from 38-71% (2). LYG is unusual from an imaging standpoint as it appears as an aggressive malignancy, but areas of involvement can spontaneously regress without being treated.
Steven Herber MD, Gabriel Swenson MD, Clinton Jokerst MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
References
- Melani C, Jaffe ES, Wilson WH. Pathobiology and treatment of lymphomatoid granulomatosis, a rare EBV-driven disorder. Blood. 2020 Apr 16;135(16):1344-1352. [CrossRef] [PubMed]
- Katzenstein AL, Doxtader E, Narendra S. Lymphomatoid granulomatosis: insights gained over 4 decades. Am J Surg Pathol. 2010 Dec;34(12):e35-48. [CrossRef] [PubMed]
- Katzenstein AL, Carrington CB, Liebow AA. Lymphomatoid granulomatosis: a clinicopathologic study of 152 cases. Cancer. 1979 Jan;43(1):360-73. [CrossRef] [PubMed]
- Nicholson AG, Wotherspoon AC, Diss TC, et al. Lymphomatoid granulomatosis: evidence that some cases represent Epstein-Barr virus-associated B-cell lymphoma. Histopathology. 1996 Oct;29(4):317-24. [CrossRef] [PubMed]
 Post a Comment
Post a Comment
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Reader Comments