
October 2024 Medical Image of the Month: Lofgren syndrome with Erythema Nodosum
 Figure 1. 3 photographs of the patient’s lower extremities demonstrating bilateral ankle swelling with erythema and warmth and an erythematous nodule over the medial right knee (middle image). To view Figure 1 in a separate, enlarged window click here.
Figure 1. 3 photographs of the patient’s lower extremities demonstrating bilateral ankle swelling with erythema and warmth and an erythematous nodule over the medial right knee (middle image). To view Figure 1 in a separate, enlarged window click here.
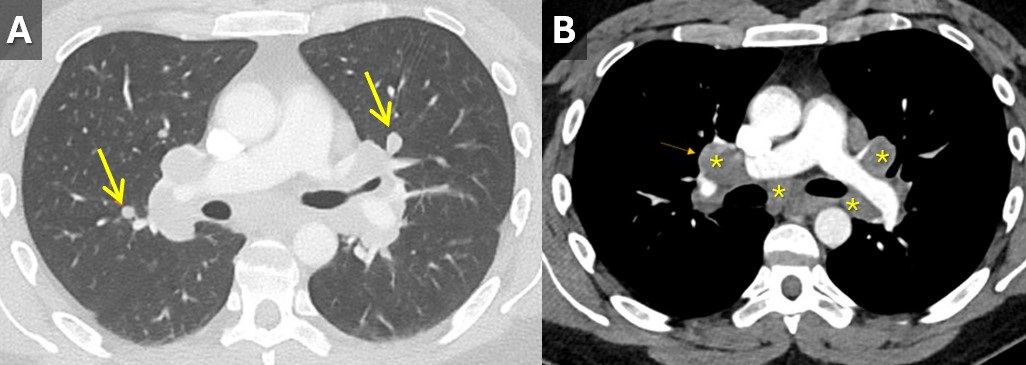
 Figure 2. Contrast-enhanced chest CT with lung (A) and soft tissue(B) windows demonstrating small scattered pulmonary nodules (arrows) and mediastinal and hilar lymphadenopathy (*). To view Figure 2 in a separate, enlarged window click here.
Figure 2. Contrast-enhanced chest CT with lung (A) and soft tissue(B) windows demonstrating small scattered pulmonary nodules (arrows) and mediastinal and hilar lymphadenopathy (*). To view Figure 2 in a separate, enlarged window click here.
A 33-year-old man with a past medical history of non-metastatic right sided testicular cancer status post radical orchiectomy 10 years prior presented to the emergency department for 1 week of bilateral lower extremity swelling and pain. He had associated shortness of breath, right sided chest pain, fatigue, and night sweats. Physical exam revealed bilateral ankle swelling with erythema and warmth and there was noted an erythematous nodule over the medial right knee and anterior right thigh (Figure 1). He was tachycardic to a rate of 110 bpm, but otherwise had an unremarkable physical exam and review of systems.
The lower extremity lesions were consistent with erythema nodosum. Sarcoidosis was an amounting differential but as this is a diagnosis of exclusion, alternate causes needed to be ruled out. Deep vein thrombosis was excluded. CT angiogram did not show pulmonary embolus but it did show diffuse multifocal sub centimeter pulmonary nodules measuring up to 8 mm with mediastinal and hilar lymphadenopathy (Figure 2). Coccidioides serologies were negative. Bronchoscopy with EBUS-TBNA showed granulomatous inflammation, and no malignancy. After exclusion of other causes, multidisciplinary discussion concluded Lofgren syndrome in the setting of sarcoidosis.
Lofgren syndrome is characterized by erythema nodosum, shortness of breath, and bilateral hilar lymphadenopathy and is a clinical syndrome of sarcoidosis. It is highly specific for sarcoidosis, and in many cases, it can be diagnostic and tissue sampling is not recommended for diagnosis unless to rule out other causes such as malignancy or infection (1). Lofgren syndrome is typically self-limiting and does not require chronic treatment, however, in the acute phase, patients can be very symptomatic and may require a short course of glucocorticoids.
Mary Jamison, NP-C
Department of Medicine
Banner University Medical Center, Tucson
Tucson, AZ USA
Reference
- Crouser ED, Maier LA, Wilson KC, et al. Diagnosis and Detection of Sarcoidosis. An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2020 Apr 15;201(8):e26-e51. [CrossRef] [PubMed]
 Post a Comment
Post a Comment{kind=link}
{kind=link}
Reader Comments