
November 2024 Imaging Case of the Month: A Recurring Issue
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona USA
Clinical History: A 65-year-old woman with a history of orthotopic liver transplantation 2 years earlier for non-alcoholic steatohepatitis presented to the Emergency Room for chronic fatigue, malaise, nausea and vomiting, and generalized weakness. She denies shortness of breath, hemoptysis, or productive cough. Her post liver transplant course was complicated by wound infection, biliary stricture requiring ERCP with stent placement, and Clostridium difficile colitis. Prior to her liver transplant the patient had chronic renal insufficiency which has been slowly progressing (creatinine of 2.8 mg/dL, estimated GFR of 17.6 mL) and she was currently undergoing renal transplant evaluation. The patient also has a past medical history of coronary artery disease requiring bypass grafting surgery, hypothyroidism requiring hormone replacement, and type II diabetes not requiring specific therapy. Her past surgical history included cholecystectomy and hysterectomy.
The patient is a lifelong non-smoker, she reports an allergy to penicillin and amoxicillin (hives), and she does not drink alcohol, and denies illicit drug use. Her medications include tacrolimus, mycophenolic acid, allopurinol, calcium, vitamin D, levothyroxine, pantoprazole, sertraline, fluconazole, sulfamethoxazole and trimethoprim, and prednisone.
On physical examination the patient was febrile (39.2º C). Her blood pressure was initially 97/53 mmHg; however, during her stay in the Emergency Department went as low as 71/41 mmHg. Her heart rate remained in the low to mid 90s, her respiratory rate was 12-14 breaths per minute, and her oxygen saturations were 99% on room air. The patient had uniformly decreased breath sounds bilaterally but the lungs were otherwise clear. Her cardiac examination was normal aside from trace bilateral pedal edema. Her abdominal examination was normal. She was neurologically intact.
A complete blood count showed a normal white blood cell count at 6.2 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 3.65 x 109/L (normal, 1.4 – 6.6 x 109/L); the percent distribution of lymphocytes, monocytes, and eosinophils was normal. Her hemoglobin and hematocrit values were 10 gm/dL (normal, 13.2 – 16.6 gm/dL) and 33.7% (normal, 34.9 – 44.5%). The platelet count was normal at 134 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal, including an albumin level at 4.3 gm/dL (normal, 3.5 – 5 gm/dL), with normal alanine aminotransferase at 42 U/L (normal, 7-45 U/L) and aspartate aminotransferase of 40 U/L (normal, 8-43 U/L); alkaline phosphatase levels, bilirubin, and coagulation studies were normal. SARS-CoV-2 PCR testing was negative.
Frontal chest radiography (Figure 1) was performed.
 Figure 1. Frontal (A) and lateral (B) chest radiography obtained in the Emergency Room. To view Figure 1 in a separate enlarged window, click here.
Figure 1. Frontal (A) and lateral (B) chest radiography obtained in the Emergency Room. To view Figure 1 in a separate enlarged window, click here.
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the second of twelve pages)
- Frontal chest radiography shows unremarkable findings
- Frontal chest radiography shows a moderate-to-large right pleural effusion
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pneumothorax
- Frontal chest radiography shows numerous small nodules
 Post a Comment
Post a Comment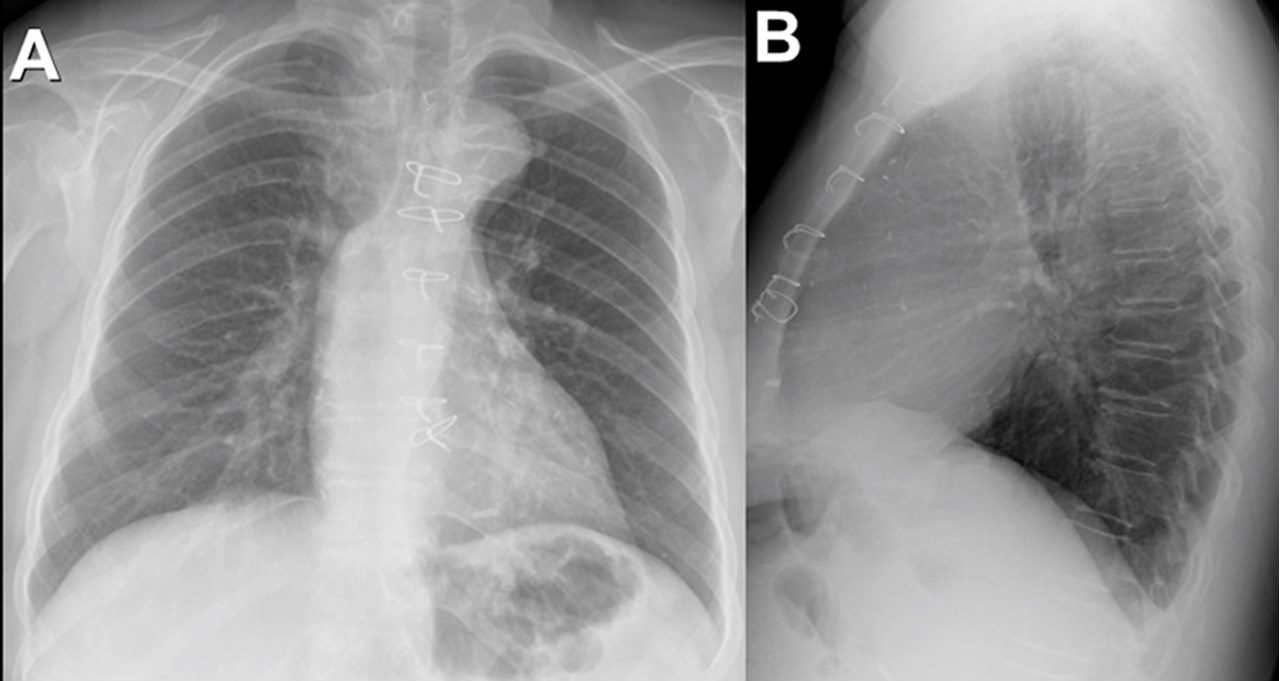{kind=link}
Reader Comments