
November 2024 Medical Image of the Month: A Case of Short Telomeres
 Figure 1. PA (A) and lateral (B) CXR demonstrating small lung volumes with peripheral reticulonodular opacities. The findings are highly suggestive of pulmonary fibrosis. To view Figure 1 in a separate, enlarged window click here.
Figure 1. PA (A) and lateral (B) CXR demonstrating small lung volumes with peripheral reticulonodular opacities. The findings are highly suggestive of pulmonary fibrosis. To view Figure 1 in a separate, enlarged window click here.
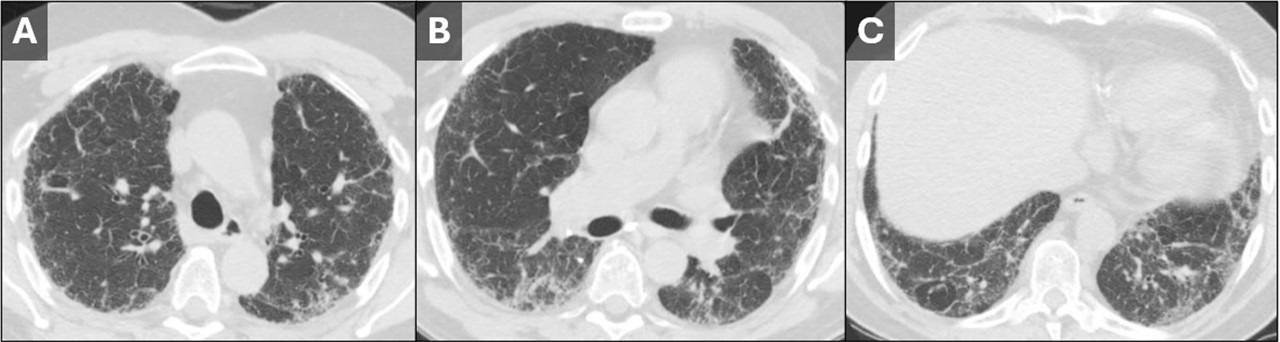
 Figure 2. Axial CT images from the upper (A), mid (B), and lower lungs (C). Images demonstrate a rather nonspecific pattern of fibrosis consisting of patchy areas of reticulation, ground glass, and septal line thickening. The findings are peripheral-predominant, but there was no predilection for the lung bases vs. apices. No subpleural honeycombing was seen. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Axial CT images from the upper (A), mid (B), and lower lungs (C). Images demonstrate a rather nonspecific pattern of fibrosis consisting of patchy areas of reticulation, ground glass, and septal line thickening. The findings are peripheral-predominant, but there was no predilection for the lung bases vs. apices. No subpleural honeycombing was seen. To view Figure 2 in a separate, enlarged window click here.
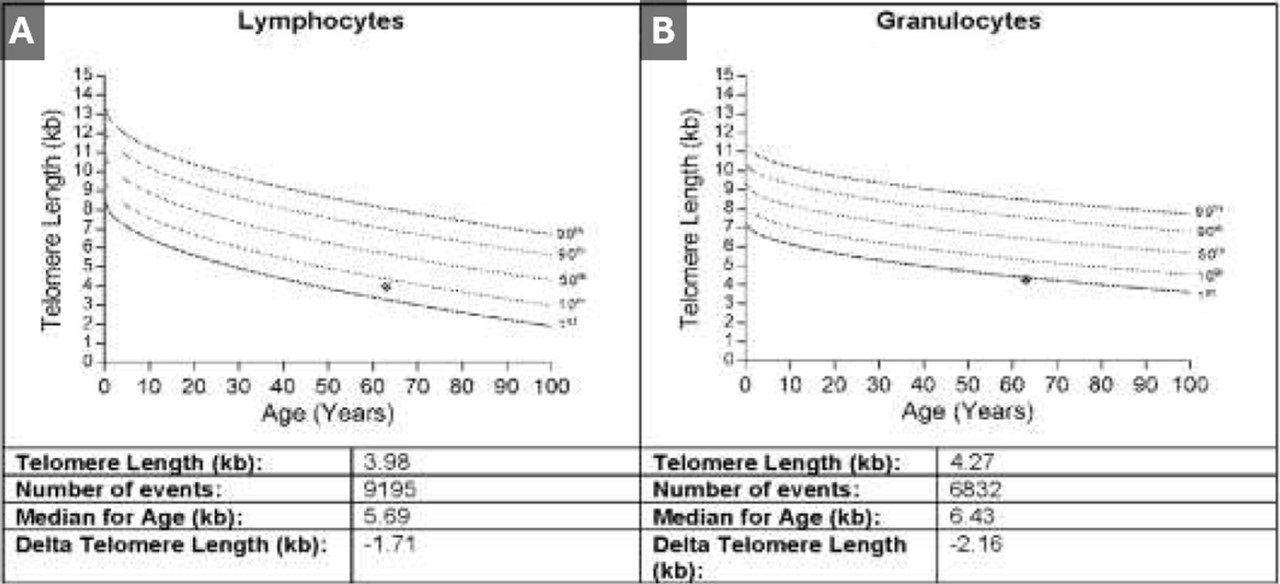
 Figure 3. Results from telomere length testing of lymphocytes (A) and granulocytes (B). The results of both tests put the patient below the 10th percentile with the granulocyte telomere length being below the 1st percentile. To view Figure 3 in a separate, enlarged window click here.
Figure 3. Results from telomere length testing of lymphocytes (A) and granulocytes (B). The results of both tests put the patient below the 10th percentile with the granulocyte telomere length being below the 1st percentile. To view Figure 3 in a separate, enlarged window click here.
A 50-year-old woman was referred to our institution for further evaluation of her ILD. Her history of present illness began during the COVID-19 pandemic, when she noticed that she had trouble climbing stairs while wearing a mask. She also had a slowly progressive cough which, at first, she attributed to seasonal allergies. Eventually her symptoms prompted pulmonary function testing at an outside institution, which showed moderately severe restriction with a DLco 40% of predicted. Chest x-ray (Figure 1) and chest CT (Figure 2) demonstrated findings of pulmonary fibrosis. The patient worked as an accountant and was a life-long nonsmoker. No concerning exposure history and no history of any medications associated with pulmonary fibrosis. Her family history is remarkable for a brother diagnosed with IPF at age 49, currently status post lung transplant. Her sister and father were both diagnosed with alpha-1-antitrypsin (both died in their 50’s). The patient also reports premature graying of her hair, at age 17. The combination of family history, gray hair, and pulmonary fibrosis prompted further testing for short telomeres, which was positive (Figure 3). The patient was diagnosed with interstitial lung disease secondary to short telomere syndrome.
Telomeres are short repeating nucleotides that the end of chromosomes that protect them from gradual degradation during aging (1). Short telomere syndromes (STSs) are accelerated-aging syndromes often caused by heritable gene mutations that result in decreased telomere length. Organ systems with increased cell turnover, such as skin, lungs, bone marrow, and GI tract, are most commonly affected (2). The relationship between telomere length and interstitial lung disease is complicated. The first association between genetically determined telomere abnormalities and lung fibrosis was observed for the telomeropathy dyskeratosis congenital (DC), an entity characterized by skin abnormalities, bone marrow failure, and pulmonary fibrosis, which was observed in 19% of patients (3). Mutations in other telomere related genes have subsequently been identified in familial and sporadic idiopathic interestitial pneumonias (4-6). Short telomeres have been identified in about 25 percent of sporadic cases of IPF (7) and should be suspected in patients with familial pulmonary fibrosis and/or early onset IPF in patients with signs of premature aging, such as developing gray hair at a young age.
Clinton E. Jokerst MD, Matthew T. Stib MD, Carlos A. Rojas MD, Michael B. Gotway MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
References
- Martínez P, Blasco MA. Telomere-driven diseases and telomere-targeting therapies. J Cell Biol. 2017 Apr 3;216(4):875-887. [CrossRef] [PubMed]
- Mangaonkar AA, Patnaik MM. Short Telomere Syndromes in Clinical Practice: Bridging Bench and Bedside. Mayo Clin Proc. 2018 Jul;93(7):904-916. [CrossRef] [PubMed]
- Knight S, Vulliamy T, Copplestone A, Gluckman E, Mason P, Dokal I. Dyskeratosis Congenita (DC) Registry: identification of new features of DC. Br J Haematol. 1998 Dec;103(4):990-6. [CrossRef] [PubMed]
- Cronkhite JT, Xing C, Raghu G, Chin KM, Torres F, Rosenblatt RL, Garcia CK. Telomere shortening in familial and sporadic pulmonary fibrosis. Am J Respir Crit Care Med. 2008 Oct 1;178(7):729-37. [CrossRef] [PubMed]
- Diaz de Leon A, Cronkhite JT, Katzenstein AL, et al. Telomere lengths, pulmonary fibrosis and telomerase (TERT) mutations. PLoS One. 2010 May 19;5(5):e10680. [CrossRef] [PubMed]
- Newton CA, Batra K, Torrealba J, et al. Telomere-related lung fibrosis is diagnostically heterogeneous but uniformly progressive. Eur Respir J. 2016 Dec;48(6):1710-1720. [CrossRef] [PubMed]
- Armanios MY, Chen JJ, Cogan JD, et al. Telomerase mutations in families with idiopathic pulmonary fibrosis. N Engl J Med. 2007 Mar 29;356(13):1317-26. [CrossRef] [PubMed]
 Post a Comment
Post a Comment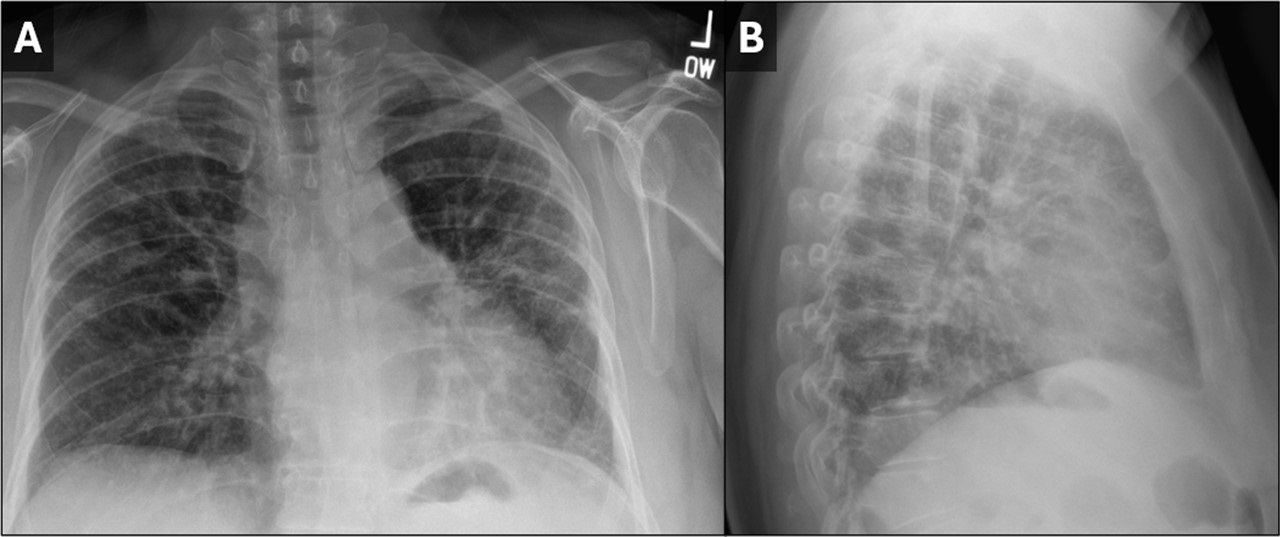{kind=link}
{kind=link}
{kind=link}
Reader Comments