Infected Chylothorax: A Case Report and Review
Louis Eubank1, Luke Gabe1, Monica Kraft1, and Dean Billheimer2
1Departments of Medicine and Biostatistics, College of Medicine
2Department of Biostatistics, College of Public Health
University of Arizona Health Sciences Center
Tucson, AZ USA
Abstract
Infected chylothorax is a rare complication of a rare pathology with limited literature entirely consisting of case reports, meeting abstracts, and letters to the editor. The case of a 56-year-old male with a spontaneous infected chylothorax successfully treated and discharged to home without any residual effects is described. A systematic review of the literature revealed 11 prior cases of infected chylothoraces. Their etiologies (when known), initial pleural fluid values, and treatment are described. These cases show that while infected chylothorax has a varied presentation and affects a broad range of patients, conservative management including antibiotics, pleural fluid drainage, and symptomatic relief is a safe and appropriate starting point.
Introduction
Chylothorax, a pleural effusion caused by chyle accumulation from obstruction or disruption of the thoracic duct (please see SWJPCC’s Image of the week: chylothorax for an image of non-infected chyle fluid), is a rare condition that may arise from a diversity of etiologies broadly categorized as traumatic or non-traumatic/spontaneous (1). Traumatic causes commonly include iatrogenic injury and chest trauma, although insults as minor as sneezing, light exercise and emesis have been reported (1-3). Non-traumatic chylothorax has been linked to several immunologic and infectious etiologies (1). Regardless of the underlying mechanism, chyle has classically been considered inherently bacteriostatic (1). We present a case of spontaneous infected chylothorax and the first review of infected chylothoraces reported in the literature.
Case Report
A 56-year-old man with alcoholic cirrhosis and remote right-sided hepatic hydrothorax presented to the emergency department complaining of shortness of breath. Patient reported slowly worsening dyspnea over the last six weeks without any other symptoms that had acutely worsened on morning of presentation
Initial vital signs were temperature 38.0°C, heart rate 115, blood pressure 81/60mmHg, and respiratory rate 30 breaths/min on 4L O2 by nasal cannula; labs significant for white blood cell count of 3100/mm3 and lactate 5.0 mmol/L (normal <2.0 mmol/L). Physical exam demonstrated a fatigued patient with accessory muscle use on inspiration and absent breath sounds at the left lung base. Computed tomography (CT) study of the chest showed a large free-flowing left-sided pleural effusion (Figure 1A&B) as well as subacute rib fractures (Image 1C).

Figure 1. Thoracic CT on the day of presentation. Panel A: Axial view showing pleural effusion. Panel B: Sagittal view showing pleural effusion. Panel C: Coronal view showing rib fractures (white arrows).
Chart review demonstrated an emergency department visit five months previously for a fall with acute left-sided rib fractures and minimal left-sided pleural effusion.
Thoracentesis removed two liters free-flowing, brown, milky, purulent fluid; analysis significant for 58,880 total nucleated cells (32,800 RBCs), 94% neutrophils, glucose <5, LDH 573 IU/dL (serum 193 IU/dL), triglycerides 191 mg/dL, albumin 1.8 g/dL (serum albumin 2.6 g/dL, laboratory lower limit of normal 3.4 g/dL).
The patient remained hypotensive despite fluid boluses, tachypneic with increasing oxygen requirements, and a repeat lactate was 6.4 mmol/L. Norepinephrine and broad-spectrum antibiotics were started and patient was admitted to the intensive care unit.
Pleural fluid and blood cultures grew Escherichia coli resistant to fluoroquinolones. Chest x-ray showed persistent pleural effusion; a chest tube was placed which drained an additional 1.6 L over the following 24 hrs. The patient subsequently improved: serum lactate normalized within 24 hours, vasopressors were weaned within 36 hours, and supplemental oxygen was discontinued within 72 hours.
Chest tube output decreased to less than 200 ml/day within 48 hours of placement; however, repeat thoracic CT demonstrated a persistent multi-loculated left pleural effusion. Surgical evacuation and pleurodesis were considered given the lack of literature regarding intrapleural lytic therapy in infected chylothorax (a single case report described use of streptokinase in a persistent non-infected chylothorax, 1). However, the patient’s operative risk was considered prohibitively high. He was managed conservatively with a fat-free diet to reduce chyle leak.
Eleven days after initial presentation fluid studies were significant for triglyceride 45mg/dL with negative cultures. Given that a pleural fluid triglyceride level <50mg/dL yields a less than 5% likelihood of being chylous and the clinical stability of the patient, the chylothorax was felt to be resolved (1). The patient was discharged to home twelve days after initial presentation.
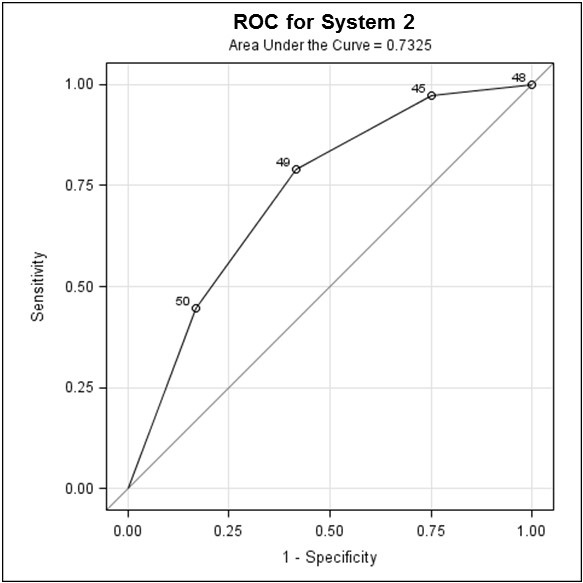
The etiology of patient’s infected chylothorax was never fully elucidated. The most likely explanation is the trauma causing rib fractures also caused a traumatic chylothorax that later became infected. The thoracic duct lies alongside the vertebrae until it drains into the left brachiocephalic vein (Figure 2).

Figure 2. Thoracic duct anatomy (black arrows).
A blow to the posterior left thorax sufficient to fracture multiple ribs is more than sufficient to damage the nearby thoracic duct (1-4). Arguing against this is most patients with large traumatic chylothoraces present within 10 days of injury (1,2).
Another explanation is the patient developed bacterial empyema secondary to hepatic hydrothorax (ascites that has passed through diaphragm from the peritoneal cavity) followed by non-traumatic chylothorax. These empyemas can demonstrate an indolent course and Escherichia coli is one of the most common causative pathogens isolated (1). Arguing against this is the patient’s previous hepatic hydrothorax was right-sided.
Finally, the chylothorax may have arisen from one of the many known causative medical pathologies (2). Chylous ascites secondary to cirrhosis that migrates into the pleural space via diaphragmatic leaks defects is a known phenomenon, albeit extremely rare (2).
In follow-up two months after discharge the patient had total resolution of respiratory symptoms and no recurrence of the effusion.
Systematic Review
Methods
A MEDLINE search (PubMed) from January 1975 to January 2018 and a Google Scholar search (all years) was conducted to identify eligible studies using the following terms: “Infected Chylothorax” (all fields) OR “Infection AND Chylothorax” (all fields) OR “Chylothorax AND Empyema” (all fields) OR “Chylous Empyema” (all fields). The inclusion criteria for studies were patients with infected non-traumatic chylothorax. A triglyceride level > 110 mg/dL or the presence of chylomicrons in pleural fluid was used to confirm the diagnosis of chylothorax; pleural fluid culture speciation was used to confirm the infection. The exclusion criteria were a lack of laboratory data and duplicate data. Two reviewers (LE, LG) independently reviewed the titles, abstracts, and, when necessary, the full text regarding the inclusion/exclusion criteria. Data extraction was performed independently by two reviewers (LE, LG) using data extraction forms defined beforehand. Discrepancies were resolved by consensus discussion with a third reviewer (MK).
Results
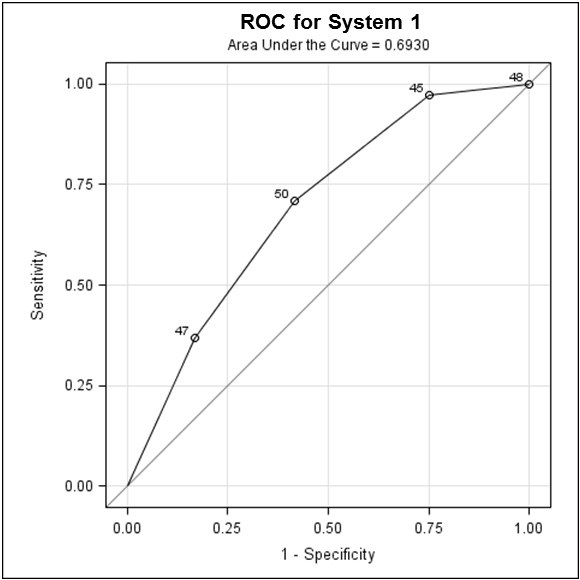
Eight case reports, two published abstracts, and one letter to the editor met the inclusion criteria; all eleven were included in the analysis (Figure 3, 13-23).

Figure 3. Flow diagram of the literature review.
The general characteristics, demographics, and etiology of infected chylothorax are summarized in Table 1, the initial pleural fluid values are reported in Table 2.
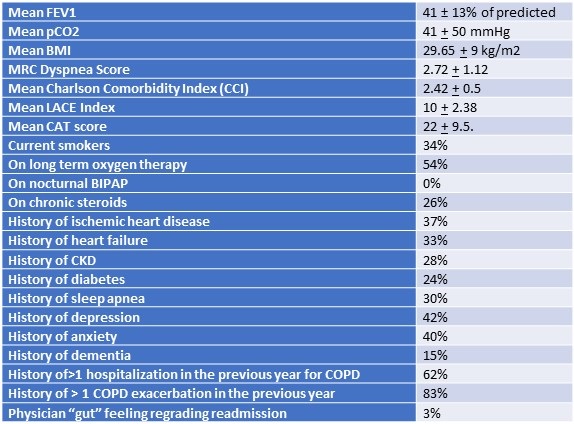
Table 1. Population data.

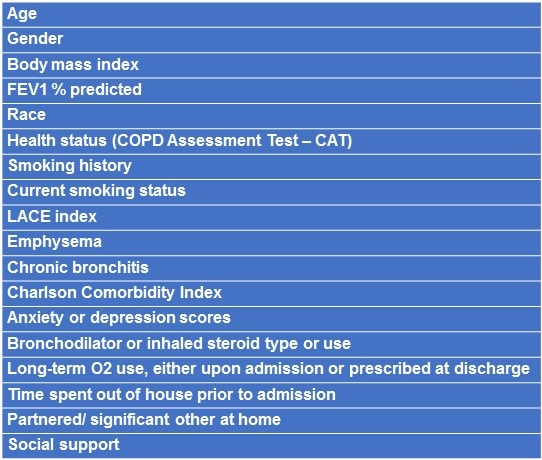
Table 2. Initial pleural fluid values.

There were 11 patients total: six males and five females; age range 5 days-78 years, mean age 40.5 years (standard deviation 28.5 years). One patient was pharmacologically immunosuppressed while others had chronic diseases known to reduce immune system function including diabetes, excessive alcohol intake, and obesity (24-26). Four (36%) were iatrogenic. Three patients (27%) were infected with Streptococcus viridans and five (45%) were infected with Streptococcus genus. In those with available data, three of ten patients (30%) required intravenous vasopressors. No patients required ventilator management for their chylothorax (two patients were already intubated, one for acute respiratory distress syndrome, the other for unstable hemodynamics secondary to large subarachnoid hemorrhage). Two patients (18%) were managed surgically – one was specifically noted to have failed conservative management (17). Of the known outcomes, eight of nine (89%) survived to discharge and all eight remained asymptomatic at follow-up. The mean follow-up duration was 13.3 months (range 6-24 months).
Discussion
Given the paucity of published experience regarding infected chylothoraces, we believe a descriptive summary is warranted. First, there is a large variation in patient characteristics, including age range, immune competence, comorbid medical conditions, and infectious organism (eight different bacterial species and one parasite).
Second, many of the reviewed cases had a more benign presentation than might be anticipated in the context of a large, infected intrathoracic fluid collection. Seven of the patients (73%) were hemodynamically stable on presentation and the majority of these patients had very mild chief complaints.
Third, the available data suggest a surprisingly good prognosis considering a previously estimated morality of 10-25% in non-infected chylothoraces, depending on etiology (27). The one patient who did not survive to discharge died due to brain herniation. Those with documented outpatient follow-up were asymptomatic up to 16 months post-discharge.
Fourth, conservative management was frequently efficacious. Eight patients (73%) were medically managed without complication and did not require extensive antibiotic duration, intrapleural lytic therapy, or surgical intervention. The decision to pursue surgical intervention is not well defined given the very limited number of cases requiring surgical management. A brief discussion of non-infected chylothoraces and their management is therefore warranted.
Non-infected chylothorax is universally described as a rare event, although its exact incidence has not been described. Chylous ascites, which sometimes shares pathogenesis with chylothorax and is one of the causes of spontaneous chylothorax, has an occurrence of one in 20,000 hospital admissions (12). Trauma accounts for approximately 50% of chylothoraces, with esophagectomy being the most common iatrogenic cause (28). Thirty percent are due to malignancy; lymphoma accounts for 70-75% of malignant cases (11). While there are no consensus guidelines on how to treat chylothoraces, many authors agree that first line treatment is conservative management with thoracentesis or chest tube drainage, fat free or medium chain triglyceride diet, and consideration of somatostatin or octreotide (1,5,11,27-29). Although somatostatin or octreotide are used at many institutions, data regarding indications & efficacy of these medications are limited and/or inconsistent – some institutions use these medications at the beginning of treatment, others only if/when initial management has failed (5,27).
Additional treatments may depend on the etiology of the chylothorax: it is suggested that earlier surgical intervention in iatrogenic traumatic chylothoraces, especially post-esophagectomy, may be beneficial (30). Conservative management is likely to fail and surgical intervention is recommended in the following situations: 1) daily drainage greater than 1000 mL chyle (adults) or greater than 100mL chyle/kg body weight (children); 2) chyle leak that persists for more than 14 days; 3) unchanged chest tube output for 7-14 days; 4) clinical deterioration (27,28).
Conservative management for infected chylothoraces appears efficacious in our small sample size with the obvious modification of treating the infection. Most antibiotics adequately penetrate the pleural space, although aminoglycosides should be avoided as they appear to be inactivated by the low pH and relative anaerobic conditions (31).
Limitations
The limitation of this systematic review was the inclusion of only case reports, abstracts, and letters to the editor and the small sample size. Unfortunately, given the rarity of infected chylothoraces, studies with sufficient sample size are unlikely to be available.
Conclusion
Infected chylothorax is a rare complication of an already rare pathology. Our case report and literature review show that it can affect any age group, can be caused by several different organisms, and has a variable presentation. Our data suggests that an initial conservative management strategy in infected chylothoraces can be a safe and effective option.
References
- McGrath E, Blades Z, Anderson P. Chylothorax: aetiology, diagnosis and therapeutic options. Respir Med. 2010;104:1-8. [CrossRef] [PubMed]
- García-Tirado J, Landa-Oviedo HS, Suazo-Guevara I. Spontaneous bilateral chylothorax caused by a sneeze: an unusual entitiy with good prognosis. Arch Bronconeumol. 2017 Jan;53(1):32-3. [CrossRef]
- Torrejais JC, Rau CB, de Barros JA, Torrejais MM. Spontaneous chylothorax associated with light physical activity. J Bras Pneumol. 2006 Nov-Dec;32(6):599-602. [CrossRef] [PubMed]
- Rodrigues AL, Romaneli MT, Ramos CD, Fraga AM, Pereira RM, Appenzeller S, Marini R, Tresoldi AT. Bilateral spontaneous chylothorax after severe vomiting in children. Rev Paul Pediatr. 2016 Dec;34(4):518-521. [PubMed]
- Bender B, Murthy V, Chamberlain RS. The changing management of chylothorax in the modern era. Eur J Cardiothorac Surg. 2016 Jan;49(1):18-24. [CrossRef] [PubMed]
- Verma SK, Karmakar S. Hodgkin's lymphoma presenting as chylothorax. Lung India. 2014 Apr-Jun; 31(2):184-6. [CrossRef] [PubMed]
- Kuan YC, How SH, Ng TH, Abdul Rani MF. Intrapleural streptokinase for the treatment of chylothorax. Respir Care. 2011 Dec;56(12):1953-5. [CrossRef] [PubMed]
- Nair SK, Petko M, Hayward M. Aetiology and management of chylothorax in adults. Eur J Cardiothorac Surg. 2007 Aug;32(2):362-9. [CrossRef] [PubMed]
- Pillay TG, Singh B. A review of traumatic chylothorax. Injury. 2016 Mar;47(3):545-50. [CrossRef] [PubMed]
- Tu CY, Chen CH. Spontaneous bacterial empyema. Curr Opin Pulm Med. 2012 Jul;18(4):355-8. [CrossRef] [PubMed]
- Skouras V, Kalomenidis I. Chylothorax: diagnostic approach. Curr Opin Pulm Med. 2010 Jul;16(4):387-93. [CrossRef] [PubMed]
- Tsauo J, Shin JH, Han K, Yoon HK, Ko GY, Ko HK, Gwon DI.Transjugular intrahepatic portosystemic shunt for the treatment of chylothorax and chylous ascites in cirrhosis: a case report and systemic review of the literature. J Vasc Interv Radiol. 2016 Jan;27(1):112-6. [CrossRef] [PubMed]
- Bensoussan AL, Braun P, Guttman FM. Bilateral spontaneous chylothorax of the newborn. Arch Surg. 1975 Oct;110(10):1243-5. [CrossRef] [PubMed]
- Asnis DS, Saltzman HP, Iakovou C, Byrns DJ. Anaerobic empyema and chylothorax. Inf Dis Clin Pract. 1994;3(5):368-70. [CrossRef]
- Natrajan S, Hadeli O, Quan SF. Infected spontaneous chylothorax. Diagn Microbiol Infect Dis. 1998 Jan;30(1):31-2. [CrossRef] [PubMed]
- Guarracino JF, Murruni A; Basílico H, Villasboas RM, Halabe K, Barroso S, Demirdjian G. Chylothorax: Unusual complication presented in a burned child with an inflation injury under the effects of mechanical ventilation (Originial title Quilotórax: Complicación pocofrecuente en un ni-o quemado en asistencia respiratoria mecánica por síndrome inhalatorio). Revista Argentina de Burns 2000:15 (1). Available at: http://www.medbc.com/meditline/review/raq/vol_15/num_1/text/vol15n1p30.htm (accessed 8/24/18).
- Wang JT, Hsueh PR, Sheng WH, Chang SC, Luh KT. Infected chylothorax caused by Streptococcus agalactiae: a case report. J Formos Med Assoc. 2000 Oct;99(10):783-4. [PubMed]
- Biswas A, Ghosh JK, Chatterjee A, Basu K, Chatterjee S. Infected chylothorax caused by escherichia coli in a non-immunocompromised child. Indian J Pediatr. 2008 Feb;75(2):192-3. [CrossRef] [PubMed]
- Alkassis SH, Bou Khalil BK. Infected chylothorax [abstract]. Presented at American Thoracic Society international meeting 2010 https://www.atsjournals.org/doi/abs/10.1164/ajrccm-conference.2010.181.1_MeetingAbstracts.A4591 (accessed 8/24/18).
- Epelbaum O, Kazianis J. Chylous empyema or empyematous chylothorax? [Abstract] Presented at American Thoracic Society international meeting 2011. https://www.atsjournals.org/doi/pdf/10.1164/ajrccm-conference.2011.183.1_MeetingAbstracts.A6460 (accessed 8/24/18)
- Wright RS, Jean M, Rochelle K, Fisk D. Chylothorax caused by paragonimus westermani in a native Californian. Chest. 2011 Oct;140(4):1064-6. [CrossRef] [PubMed]
- Bakar B, Pampal K, Tekkok IH. Infected bilateral chylothorax in a problematic case. Curr Surg. 2012 April;2(2):62-5. [CrossRef]
- Di Marco Berardino A, Inchingolo R, Smargiassi A, Re A, Torelli R, Fiori B, d'Inzeo T, Corbo GM, Valente S, Sanguinetti M, Spanu T. Empyema cause by prevotella bivia complicating an unusual case of spontaneous chylothorax. J Clin Microbiol. 2014 Apr;52(4):1284-6. [CrossRef] [PubMed]
- Geerlings SE, Hoepelman AI. Immune dysfunction in patients with diabetes mellitus. FEMS Immunol Med Microbiol. 1999 Dec;26(3-4):259-65. [CrossRef] [PubMed]
- Boule LA, Ju C, Agudelo M, et al. Summary of the 2016 Alcohol and Immunology Research Interest Group (AIRIG) meeting. Alcohol. 2018 Feb;66:35-43. [CrossRef] [PubMed]
- Milner JJ, Beck MA. The impact of obesity on the immune response to infection. Proc Nutr Soc. 2012 May;71(2):298-306. [CrossRef] [PubMed]
- Schild HH, Strassburg CP, Welz A, Kalff J. Treatment options in patients with chylothorax. Dtsch Arztebl Int. 2013 Nov 29;110(48):819-26. [CrossRef]
- Rudrappa M, Paul M. Chylothorax. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan. [PubMed]
- Nadolski G. Nontraumatic Chylothorax: diagnostic algorithm and treatment options. Tech Vasc Interv Radiol. 2016 Dec;19(4):286-90. [CrossRef] [PubMed]
- Misthos P, Kanakis MA, Lioulias AG. Chylothorax complicating thoracic surgery: conservative or early surgical management? Updates Surg. 2012 Mar;64(1):5-11. [CrossRef] [PubMed]
- Sahn SA. Diagnosis and management of parapneumonic effusions and empyema. Clin Infect Dis. 2007 Dec 1;45(11):1480-6. [CrossRef] [PubMed]
Cite as: Eubank L, Gabe L, Kraft M, Billheimer D. Infected chylothorax: a case report and review. Southwest J Pulm Crit Care. 2018;17(2):76-84. doi: https://doi.org/10.13175/swjpcc097-18 PDF
 Post a Comment
Post a Comment