Chloe E Grace Rose1, Joshua E Kessler1, Jennifer A Weisbrod1, Brittanie V Hoang2, Amy J Grizzle3, Jason T Hurwitz3, John N Galgiani4,5
1University of Arizona College of Pharmacy, Tucson, AZ USA; 2University of Arizona College of Science, Tucson, AZ USA; 3University of Arizona Center for Health Outcomes & PharmacoEconomic Research, Tucson, AZ USA; 4University of Arizona College of Medicine, Tucson, AZ USA; 5Banner-University Health Valley Fever Program, Tucson, AZ USA
Abstract
Background
The nonspecific symptoms of Valley fever, or coccidioidomycosis, hinders its proper diagnosis. This results in unnecessary health care costs and antibiotic usage. Thus, this study seeks to determine the coverage of the Valley fever diagnostic test as provided by Arizona insurance companies to increase early diagnosis rates.
Methods
Through scripted messaging and telephone communications, we contacted 40 health insurance companies in Arizona about their coverage of CPT 86635 (antibody diagnostic assay for Coccidioides) without prior authorization under all plan types provided in both primary and urgent care settings. If prior authorization was required, we discussed the coverage of ICD-10 codes J18.9 (pneumonia, unspecified organism), J18.1 (lobar pneumonia, unspecified organism), or L52 (erythema nodosum).
Results
Of the 40 health insurance companies contacted, 25 did not answer our inquiries, most requiring member-specific information to share coverage data. The remaining 15 companies covered Valley fever testing, of which 4 required prior authorization for the ICD-10 codes of interest. Of these 15 companies, 14 provided coverage in primary and urgent care settings, and 13 provided coverage for all available plans.
Conclusion
All payers that provided information covered Valley Fever testing. Most of the insurance companies that were unable to answer our inquiry likely cover Valley fever testing, but were unable to share information with third party inquiries. Obtaining general coverage information is difficult, which can potentially impact patient care.
Abbreviation List
- CPT: Current Procedural Terminology
- ICD: International Classification of Diseases
- ELISA: enzyme-linked immunosorbent assay
Introduction
Valley fever (i.e., coccidioidomycosis) is caused by the fungus Coccidioides and infection occurs through inhalation of the airborne fungal spores. Symptoms of Valley fever infection can be similar to those of other respiratory illnesses. While many patients who are exposed to the fungus remain asymptomatic, about a third experience pneumonia, arthralgias, and skin rashes such as Erythema nodosum, which typically last many weeks to months. A small percentage have more progressive complications such as chronic fibrocavitary pneumonia or dissemination of infection beyond the chest.
Around 150,000 infections are estimated to occur in the United States each year, mostly from Arizona and California (1). Of those infected, 50,000 may seek medical attention with 10,000 to 20,000 accurately diagnosed as Valley fever (2). Nearly two-thirds of all diagnoses nationwide originate from Arizona where Valley fever is responsible for about a quarter of all community acquired pneumonia (3,4,5). Because the symptoms of Valley fever are similar to those of other respiratory illnesses, diagnosis and treatment is often delayed if a laboratory diagnosis is not pursued, most commonly by a simple blood test. For this reason, national guidelines recommend that patients should be tested for Valley fever if they have symptoms of pneumonia or Erythema nodosum and either live in or have recently travelled to areas where Coccidioides is found.
In addition to problems with under-diagnosing, there can also be long delays in reaching a diagnosis. It has been estimated that 43% of Valley fever cases take longer than one month to diagnose (6). A 2021 study reported that of 1,287 new Valley fever cases, only 12% were diagnosed in the primary care setting, and less than 1% in urgent care (7). The majority of cases were unnecessarily diagnosed during an average three-day hospital stay after patients received 14 antibiotic doses, contributing to increases in both bacterial resistance and healthcare costs (7). Promoting awareness of Valley fever testing, specifically in urgent care and primary care settings where patients often present due to symptoms, is important in order to avoid delays in diagnosis and treatment, especially in endemic areas.
Increasing Valley fever diagnosis rates could have numerous benefits. Routine serology testing in patients who are suspected to have pneumonia would help increase Valley fever diagnosis, and reduce antibiotic use, which is often used empirically in these patients without effect, since Valley fever is a fungal infection and does not respond to antibiotics. Some of the excess costs associated with Valley fever are due to long delays to identify Valley fever. Reductions in unnecessary healthcare costs due to repeated primary and urgent care visits, and hospital admissions could be expected. Lifetime costs for the 10,359 cases of Valley fever diagnosed in Arizona in 2019 were estimated at $736 million (8). This represents a potentially important target that could lead to cost savings for patients and the healthcare system.
The purpose of this research is to determine coverage of the diagnostic test for Valley fever by insurance payers in Arizona. This is in response to the frequently asked question by both patients and clinicians regarding whether testing would incur out-of-pocket costs, and thus be declined by patients. Findings from this research will inform healthcare providers about coverage of the Valley fever test in Arizona to help increase early diagnosis of Valley fever, improve patient outcomes, and reduce healthcare costs (7).
Methods
Design
This is a descriptive study designed to determine payer coverage of Valley fever diagnostic tests. We used scripted messaging and telephone communications to contact payer organizations directly. All communications aimed to answer the question: is the Current Procedural Terminology (CPT) code 86635, an antibody diagnostic assay for Coccidioides, covered without prior authorization in primary and urgent care settings? CPT codes refer to a set of medical codes created and maintained by the American Medical Association (AMA) to represent procedures and services. This CPT code was chosen because it encompasses all forms of Valley fever diagnostic tests, including complement fixation, immunodiffusion and enzyme-linked immunosorbent assay (ELISA).
While precise sensitivity and specificity has not been established for ELISA, it is thought to be highly specific and more sensitive than older methods (9). Serologic ELISA testing is done by reference laboratories and results are returned between two days and two weeks, depending upon the clinic’s location and procedures for send-out tests. A rapid test is available, but it requires a CLIA-certified laboratory which is not normally on site in most clinics (10). Clearly a point-of-care test would improve diagnosis.
We attempted to elucidate coverage further by inquiring about plan types, coverage settings, and specific ICD-10 diagnostic codes. Plan type was identified as all, not specified, or other. Payers that did not specify the plan type or provided coverage information for the most basic plan were assumed to cover all plans. In addition, we focused on coverage in urgent care and primary care settings, which have the greatest potential for improving diagnoses. Lastly, if coverage was dependent upon diagnosis and required prior authorization, we inquired whether ICD-10 codes J18.9 (pneumonia, unspecified organism), J18.1 (lobar pneumonia, unspecified organism), or L52 (erythema nodosum) would qualify for coverage of CPT 86635.
Study Population
We identified payers based on a list of claims for CPT 86635 retrieved from Sonora Quest Laboratories, one of Arizona’s market share leaders among clinical laboratories (11). Claims data was provided by Brian Mochon PhD, Clinical Associate Professor at the University of Arizona College of Medicine, and System Medical Director of Clinical Microbiology and Infectious Disease Serology for Banner Health and Sonora Quest Laboratories. The claims list was generated from patient visits at Banner Health facilities across Arizona. Sonora Quest Laboratories processed the samples used in Valley fever diagnoses and billed payers using CPT 86635. We used this claims list to identify payers to contact after removing duplicate payer entries and third-party claims processors.
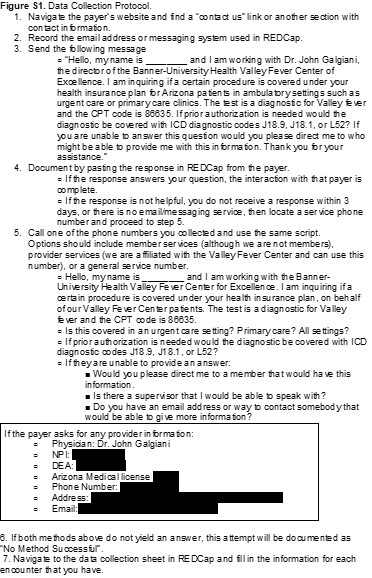
Data Collection
We used a predefined protocol to standardize the data collection process. When available, we contacted payers electronically through the use of built-in chat or messaging systems on the company websites, using a standardized message. We allowed 3 business days for a response. If they did not respond, did not provide an appropriate answer, or there was no messaging service available, we phoned the company using member or provider services. A copy of our data collection protocol is included in the supplemental materials (Figure S1).
Data collection and management used REDCap (Research Electronic Data Capture) hosted at The University of Arizona (version 11.3.4). REDCap is a secure, web-based software platform designed to support data capture for research studies (12,13). The list of variables obtained from communication with payer organizations included: payer name, method of communication used (message and telephone), department contacted, CPT 86635 coverage (including ICD-10 codes in the event of prior authorization), settings of coverage (urgent care, primary care, both), type of plan covered, and miscellaneous data including reason for non-disclosure of coverage. A copy of the complete data collection form is included in the supplemental materials (Figure S2).
Data Analysis
This is a descriptive study; no statistical significance testing was performed. Results are displayed as measures of frequency, including counts and percentages.
Results
Between 01/01/2021 and 09/21/2021 claims were submitted to 53 insurance payers. Duplicates and different plans under the same payer were merged and third-party claims processors were also excluded, resulting in 40 insurance payers for our study.
Data collection through contact with insurance companies occurred during September and October 2021. Of the 40 insurance payers identified, 12 (30.0%) had accessible online messaging via a messaging portal or email address. After messaging each of these payers with the scripted message, 6 responded. We contacted 35 (87.5%) insurance payers via telephone.
CPT 86635 was identified as covered in 15 (37.5%) of our communications (Figure 1).

Figure 1. Coverage of CPT code 86635 (Valley fever diagnostic tests) by 40 payers.
Of those 15 payers, 4 required prior authorization while 11 (73.3%) did not. All three of the ICD-10 codes (J18.1, J18.9, and L52) were accepted to obtain authorization. Those that did require prior authorization were either Department of Defense associated plans, or were not based out of Arizona, where coccidioidomycosis infections may not be as prominent.
Both the online message and phone script included differences in CPT coverage between an urgent care and primary care setting. Positive coverage responses that did not differentiate variations in coverage based on setting were recorded as covered in both urgent care and primary care. Of all positive coverages, 14 (93.3%) were covered in both urgent care and primary care and 1 (6.7%) did not specify if coverage was for both urgent care and primary care. Table 1 summarizes CPT coverage details.
Table 1. Coverage details for CPT code 86635 among payers (N = 40) a.

aList of payers (N=40) included: AARP Medicare, Aetna, All Savers, Allied Benefits System, Allwell, Ambetter, American Indian Health Program, ASR Health Benefits, AZ Foundation for Medical Care, Banner Family Care, BCBS Alabama, BCBS AZ, Bright Health, Care 1st Wellcare, CHAMP, Cigna, GEHA, Health Net, Humana, Imperial Health Texas Inc., Intel Arizona Connected Care, Kaiser Permanente, The Loomis Company, Medicare, Mercy Care, Meritain, Molina Complete Care of AZ, Multiplan Unified Life Insurance Company, OneCare Wellcare Medicare Advantage, Oscar Health Plan, Philadelphia American Life, Railroad MCR, Sierra Health and Life, Steward Health Choice, Summit, Tricare, Triwest VAPC, United Health, United Healthcare Community Plan, and WellCare MCR.
Of the 15 covered communications, 13 (86.7%) covered all plans, while 1 (6.7%) communication did not specify variation between plans, and 1 (6.7%) was member-specific to one of our researchers and denoted as “other”.
Of the 40 insurers contacted, 25 (62.5%) were unable to provide coverage information for Valley fever testing. The majority required member-specific information in order to disclose coverage details about a contracted plan. Given we had no specific patient for each plan and were only making general inquiries on behalf of a physician, we listed these communications as “Unable to Determine”. None of the 40 payers indicated that CPT code 86635 was not covered.
Discussion
In this study, we obtained coverage information for Valley fever diagnostic tests from 15 of the 40 payers we contacted. Of note, none of the remaining 25 payers said CPT code 86635 was not covered under their plans, only that they could not provide information, largely because such information requires specific member identification for one of their plan holders. In addition, 4 of the total providers required prior authorization for the diagnostic. These providers were either Department of Defense associated plans or were not based out of Arizona or California. Since coccidioidomycosis is largely endemic to Arizona and California, it is not unreasonable for an out of state insurance provider to require a prior authorization for a condition that is not endemic to their population. However, some national providers and out of state providers did state they cover the diagnostic without a prior authorization.
The difficulty of obtaining general coverage information from an insurance payer quickly became apparent. We anticipated that some payers would not disclose coverage information, however, given that we were requesting information on behalf of a practicing physician, we did not anticipate this response from most payers. The lack of transparency in providing benefit information to potential patients or providers is concerning and may negatively impact patient care. However, based upon the favorable response we received from payers that did provide information, it is likely that most of the insurers unable to provide information do cover the Valley fever diagnostic test.
Our findings build upon literature describing the lack of diagnoses of Valley fever, predominantly in the urgent care setting. Pu et al. (2020) reported the total diagnosis of coccidioidomycosis was a mere 0.5% in the urgent care setting from 2017-2019. At the time of our study, we found no previous publications on payer coverage of Valley fever diagnostic tests. However, we identified similar methods utilized in the existing literature. Cohen et al. (2019) researched insurance policies for coverage of gender re-affirming surgeries via online and telephonic methods and identified policies for 124 of 150 payers (14). A report by Park et al. (2019) researched insurance coverage policies for multiple pharmacogenomic tests via online methods and identified policies for 33 of 41 payers (15). Both of these studies were able to identify a larger proportion of coverage from the identified payers than our current study, though Park et al. (2019) did highlight difficulties from a patient or provider perspective in identifying payer coverage (13).
Results, however, must be considered in light of several study limitations. Payers were limited to those that were available via claims data from Sonora Quest Laboratories for predominantly Arizona payers. In addition, the claims data were derived solely from patients seen at Banner Health facilities, excluding patients seen for diagnosis and claims filed outside of the Banner Health network. The actual population of Valley fever patients is likely larger and may have had different coverage patterns than we collected. This data source and focus on Arizona limits generalizability of findings. However, Valley fever is endemic to Arizona and the Southwestern region of the United States.
This study also faced data collection limitations. Although our communications were scripted, the payers’ representatives may have not had a similar procedure. We may have obtained different results based upon the individual who was communicated with, and this may have impacted our ability to gather information.
For this study, we assumed that confirming CPT 86635 coverage by the payer’s representative meant coverage was generalizable to all plan types offered by the payer and all care settings where a patient might be seen. If a payer did not specify variability in coverage based on plan or care setting, we assumed all plans and all care settings were covered without need for prior authorization.
Due to barriers that often exist for patients to see a primary care provider in a timely manner, many patients’ first interaction for Valley fever is in an urgent care setting. There remains a need to educate these providers about the availability and coverage of tests for patients, as current lack of knowledge may negatively impact patient care by delaying diagnoses and potentially leading to hospitalization. While insurance coverage or cost may or may not be a limiting factor for a provider to order the diagnostic test, cost could be a limiting factor for the patient. Education can be provided to providers about recognition and testing coverage for Valley fever. Patients could then be educated as well in recognition of symptoms and insurance coverage trends, which could increase total tests ordered. Increased testing rates could help identify Valley fever diagnoses sooner and more frequently. This study highlights an important step of identifying payer coverage for Valley fever diagnosis in an urgent care setting. These results may help to inform providers about insurance coverage for their patients and increase early diagnosis of Valley fever cases. Future research could build upon this study by incorporating provider knowledge and education in relation to the impact on patients presenting with Valley fever in urgent care and primary care settings.
Acknowledgments
The authors wish to thank Banner Health and Sonora Quest Laboratories for their contributions in providing claims information for this research.
Author Contributions Statement
BVH, CEGR, JEK, and JAW contributed to data collection. CEGR, JEK, and JAW drafted the manuscript. AJG, JTH and JNG provided edits and commentary on the manuscript. All authors contributed to research design.
References
- Valley Fever Awareness. Centers for Disease Control and Prevention. Updated July 26, 2021. Accessed 12 October 2021. https://www.cdc.gov/fungal/features/valley-fever.html
- Galgiani JN. Coccidioidomycosis (coccidioides species). In: Bennett JE, Dolin R, Blaser MJ, eds. Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, 9th Ed. Philadelphia, PA: Elsevier; 2019.
- Valley Fever Statistics. Centers for Disease Control and Prevention. Accessed 12 October 2021. https://www.cdc.gov/fungal/diseases/coccidioidomycosis/statistics.html
- Kim MM, Blair JE, Carey EJ, Wu Q, Smilack JD. Coccidioidal pneumonia, Phoenix, Arizona, USA, 2000-2004. Emerg Infect Dis. 2009;15(3):397-401. doi:10.3201/eid1563.081007
- Valdivia L, Nix D, Wright M, et al. Coccidioidomycosis as a common cause of community-acquired pneumonia [published correction appears in Emerg Infect Dis. 2006 Aug;12(8):1307]. Emerg Infect Dis. 2006;12(6):958-962. doi:10.3201/eid1206.060028
- Donovan FM, Wightman P, Zong Y, et al. Delays in Coccidioidomycosis Diagnosis and Associated Healthcare Utilization, Tucson, Arizona, USA. Emerging Infectious Diseases. 2019;25(9):1745-1747. doi:10.3201/eid2509.190023.
- Pu J, Donovan FM, Ellingson K, et al. Clinician Practice Patterns That Result in the Diagnosis of Coccidioidomycosis Before or During Hospitalization. Clin Infect Dis. 2020;73(7):e1587-e1593. doi:10.1093/cid/ciaa739
- Grizzle AJ, Wilson L, Nix DE, Galgiani JN. Clinical and Economic Burden of Valley Fever in Arizona: An Incidence-Based Cost-of-Illness Analysis. Open Forum Infect Dis. 2020;8(2):ofaa623. Published 2020 Dec 28. doi:10.1093/ofid/ofaa623
- Learn More about Who We Are. Sonora Quest Laboratories. Accessed 15 October 2021. https://www.sonoraquest.com/about/who-we-are/.
- Galgiani JN, Ampel NM, Blair JE, et al. 2016 Infectious Diseases Society of America (IDSA) Clinical Practice Guideline for the Treatment of Coccidioidomycosis. Clin Infect Dis. 2016;63(6):e112-e146. doi:10.1093/cid/ciw360
- Donovan FM, Ramadan FA, Khan SA, et al. Comparison of a Novel Rapid Lateral Flow Assay to Enzyme Immunoassay Results for Early Diagnosis of Coccidioidomycosis. Clin Infect Dis. 2021;73(9):e2746-e2753. doi:10.1093/cid/ciaa1205
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377-381. doi:10.1016/j.jbi.2008.08.010
- Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: Building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
- Cohen WA, Sangalang AM, Dalena MM, Ayyala HS, Keith JD. Navigating Insurance Policies in the United States for Gender-affirming Surgery. Plast Reconstr Surg Glob Open. 2019 Dec 11;7(12):e2564. doi: 10.1097/GOX.0000000000002564. PMID: 32537307; PMCID: PMC7288898.
- Park SK, Thigpen J, Lee IJ. Coverage of pharmacogenetic tests by private health insurance companies. J Am Pharm Assoc (2003). 2020 Mar-Apr;60(2):352-356.e3. doi: 10.1016/j.japh.2019.10.003. Epub 2019 Dec 13. PMID: 31843376.
Cite as: Grace Rose CE, Kessler JE, Weisbrod JA, Hoang BV, Grizzle AJ, Hurwitz JT, Galgiani JN. Payer Coverage of Valley Fever Diagnostic Tests. Southwest J Pulm Crit Care. 2021;23(6):155-61. doi: https://doi.org/10.13175/swjpcc052-21 PDF


 Post a Comment
Post a Comment





{kind=link}
{kind=link}